

The Cranial Nerves
What they do, why they matter, and how to remember all twelve without losing your mind
There are twelve cranial nerves. They are numbered with Roman numerals, named after their function or location, classified as sensory, motor, or both, and responsible for an extraordinary range of functions — from smell to eye movement, from facial expression to the regulation of your heart rate. They are tested on every major veterinary board exam. They are examined in every neurological assessment you will perform in clinical practice. And they are, in the opinion of most first-year students, one of the most memorization-intensive subjects in the entire first year curriculum.
This article is designed to make them make sense, not just as a list, but as a system. Because once you understand what each nerve does and why it is built the way it is, the memorization becomes almost incidental. The structure follows the function. The clinical signs follow the anatomy. The whole thing becomes logical.
We will cover all twelve individually, with anatomy, clinical relevance, and a memory trick for each one. Then we will look at how to use the cranial nerve examination as a diagnostic tool — because in clinical practice, this is how you actually use what you are learning right now.
THE MNEMONIC FIRST — THEN THE UNDERSTANDING
Oh Olfactory · Oh Optic · Oh Oculomotor · To Trochlear · Touch Trigeminal · And Abducens
Feel Facial · Very Vestibulocochlear · Good Glossopharyngeal · Velvet Vagus · Ah Accessory · Heaven Hypoglossal
Type (S/M/Both): "Some Say Marry Money But My Brother Says Bad Business Marry Money"
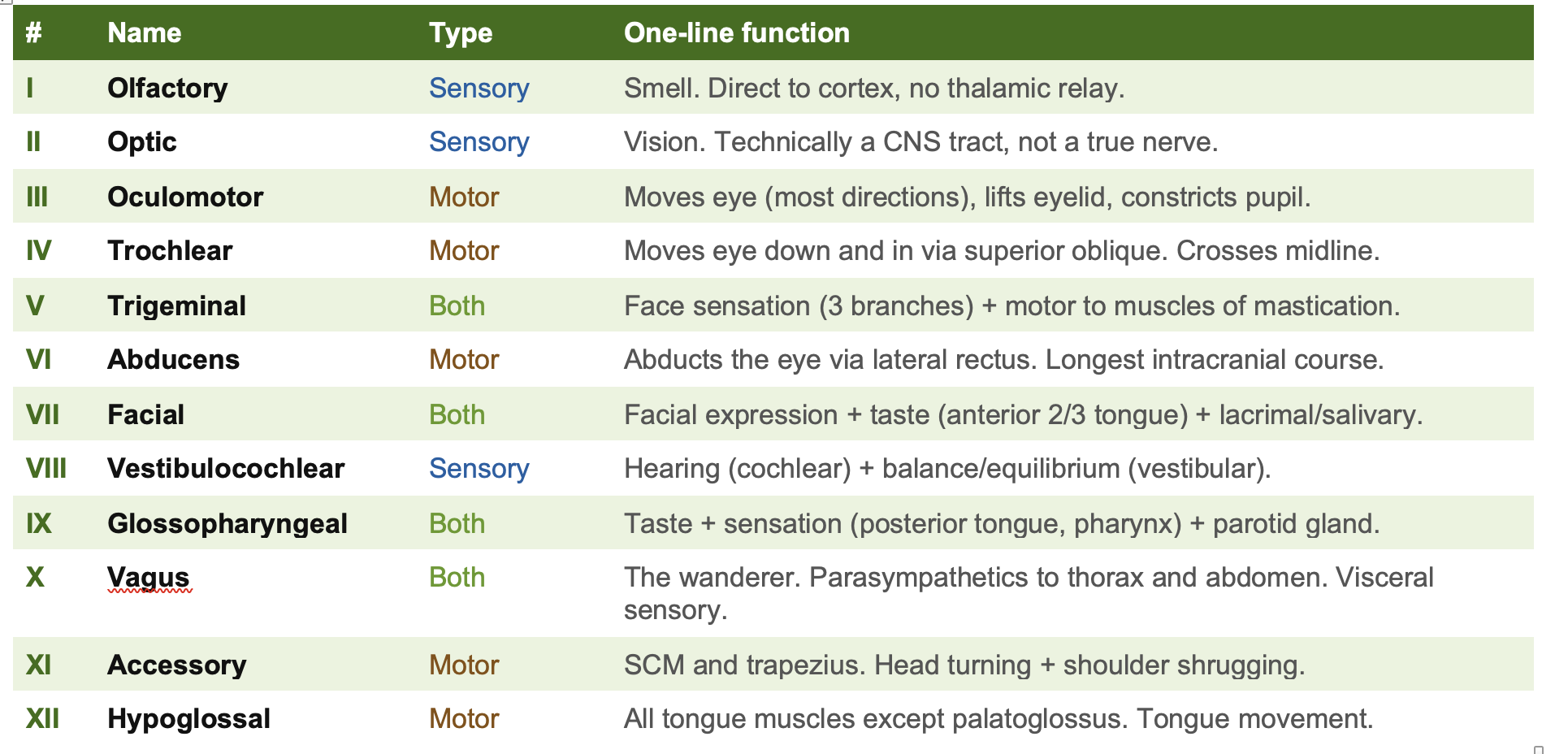
Quick Reference: All Twelve at a Glance
Color key: Blue = Sensory only, Amber = Motor only, Green = Both.
The Twelve Nerves: Full Profiles
Each nerve below includes its full anatomy, its clinical significance in both human and veterinary medicine, and a memory anchor. Read the anatomy first. Then read the clinical section. The link between structure and deficit is what makes this information durable.
I
Sensory
Olfactory — The nerve that bypasses the rules
Anatomy: The olfactory nerve is unique in that it is the only sensory system that does not relay through the thalamus before reaching the cortex. Olfactory receptor neurons in the nasal epithelium send axons through the cribriform plate of the ethmoid bone directly to the olfactory bulb. From there, projections go to the primary olfactory cortex (piriform cortex), the amygdala, and the hippocampus — which is why smells are so powerfully linked to memory and emotion. The olfactory nerve is technically a collection of approximately 20 small nerve filaments (fila olfactoria), not a single nerve trunk.
Clinical: Damage to CN I produces anosmia (loss of smell). This is clinically important because it is often the first sign of traumatic brain injury — the olfactory fila are sheared as the brain moves within the skull during deceleration injuries. Anosmia is also an early sign of several neurodegenerative diseases. In veterinary patients, loss of menace response with intact vision can sometimes indicate olfactory bulb or frontal lobe pathology rather than purely visual pathway damage.
Memory trick: One nose. First nerve. The one that goes straight to the brain and bypasses the thalamic checkpoint. Olfactory = O = One.
II
Sensory
Optic — Not technically a nerve — but on your list anyway
Anatomy: The optic nerve is embryologically and structurally a tract of the central nervous system, not a peripheral nerve. It is surrounded by meninges and contains no Schwann cells — its axons are myelinated by oligodendrocytes. Retinal ganglion cells send axons that form the optic nerve, which exits the eye at the optic disc (creating the physiological blind spot in every eye). The two optic nerves meet at the optic chiasm, where fibers from the nasal (medial) hemiretina of each eye cross to the contralateral side, while fibers from the temporal (lateral) hemiretina remain ipsilateral. This crossing pattern is the basis for the visual field deficits you will be tested on for the rest of your career.
Clinical: Visual field deficits depend precisely on lesion location. Damage before the chiasm = ipsilateral monocular vision loss. Damage at the chiasm = bitemporal hemianopia (classic sign of a pituitary mass compressing the chiasm from below). Damage after the chiasm = contralateral homonymous hemianopia. In veterinary medicine, the menace response and pupillary light reflex (PLR) both involve CN II as the afferent limb — if the PLR is present but the menace response is absent, the pathway from retina to visual cortex is disrupted somewhere beyond the optic nerve.
Memory trick: Two eyes. Second nerve. The blind spot is where CN II exits the retina. If you press on the chiasm you lose your temporal fields. The anatomy is the clinical sign.
III
Motor
Oculomotor — The nerve that moves the eye — most of it
Anatomy: CN III originates in the midbrain and travels through the cavernous sinus to the orbit via the superior orbital fissure. It supplies the superior, inferior, and medial recti, the inferior oblique, and the levator palpebrae superioris (which raises the eyelid). It also carries parasympathetic fibers from the Edinger-Westphal nucleus to the ciliary ganglion, which innervates the sphincter pupillae (pupil constriction) and the ciliary muscle (lens accommodation). The parasympathetic fibers travel on the outside of the nerve, which is clinically significant.
Clinical: A complete CN III palsy produces the classic triad: ptosis (levator paralysis), eye deviated down and out (unopposed action of CN IV and VI), and fixed dilated pupil (parasympathetic loss). Because the parasympathetic fibers are on the outside of the nerve, compressive lesions (aneurysm of the posterior communicating artery, uncal herniation) affect the pupil early. Ischemic lesions (diabetes, hypertension) tend to spare the pupil initially because the ischemia affects the core of the nerve. This distinction is clinically critical: a painful CN III palsy with pupil involvement is a neurosurgical emergency until proven otherwise.
Memory trick: CN III controls most of the eye. The number III looks like three muscle groups. Damage = down and out (the two muscles NOT supplied by CN III pull the eye). The pupil is on the outside of the nerve — compression hits it first.
IV
Motor
Trochlear — The smallest, the longest, and the only one that crosses
Anatomy: CN IV is the only cranial nerve that exits from the dorsal brainstem (all others exit ventrally). It is the cranial nerve with the longest intracranial course and the smallest number of axons. After exiting the dorsal midbrain, it wraps around the brainstem and crosses the midline before entering the cavernous sinus and passing to the orbit via the superior orbital fissure. It supplies only one muscle: the superior oblique, which depresses the eye when it is adducted (intorted and depresses the adducted eye). The action of the superior oblique is tested by asking the patient to look down and in (toward the tip of the nose).
Clinical: CN IV palsy is the most commonly missed cranial nerve palsy in clinical practice because the deficit is subtle. Patients (and veterinary patients) cannot look downward when the eye is adducted. Humans classically complain of diplopia when walking down stairs (looking down and in). They tilt their head away from the affected side to compensate — a characteristic head tilt that you will see in clinical neurology. In small animals, CN IV palsy is rarely tested in isolation but is included in neurological examinations of the eye.
Memory trick: Trochlear = Tricky. The one that crosses the midline. The one that exits from the back. The one that goes DOWN. Damage = can’t look down-and-in, tilts head to compensate.
V
Both
Trigeminal — The largest cranial nerve — sensation for the face, motor for chewing
Anatomy: CN V is the largest of the cranial nerves and has the most complex distribution. It arises from the pons and immediately divides into three branches: V1 (ophthalmic) — sensation from the forehead, upper eyelid, cornea, and nose; V2 (maxillary) — sensation from the cheek, lower eyelid, upper lip, upper teeth, and palate; V3 (mandibular) — sensation from the lower jaw, lower teeth, chin, and anterior two-thirds of the tongue, plus motor fibers to the muscles of mastication (masseter, temporalis, medial and lateral pterygoids). The corneal reflex uses V1 as its afferent limb and CN VII as its efferent limb. V3 also mediates the jaw jerk reflex.
Clinical: Loss of facial sensation in a trigeminal distribution is the hallmark of CN V pathology. Trigeminal neuralgia (tic douloureux) produces sudden, severe, electric shock-like pain in the face, classically triggered by light touch. It is one of the most painful conditions in medicine. In veterinary patients, loss of sensation in the face, inability to close the jaw (dropped jaw), or muscle atrophy over the temporalis are all signs of CN V involvement. The jaw deviates toward the affected side when the patient opens the mouth (weak pterygoids on one side allow the contralateral muscles to push the jaw across). The corneal reflex is particularly important in veterinary neurology as a way to assess brainstem function.
Memory trick: Five fingers on the face = Trigeminal covers the face. V = 5. Three branches = three territories. V3 does the chewing. Corneal reflex = V1 in, VII out.
VI
Motor
Abducens — The nerve that abducts the eye — with the longest intracranial course
Anatomy: CN VI emerges from the pontomedullary junction and has the longest intracranial course of any cranial nerve, passing over the petrous apex and through the cavernous sinus to reach the orbit via the superior orbital fissure. It supplies only one muscle: the lateral rectus, which abducts the eye (moves it temporally). Abduction of the eye is the action that is directly tested when you ask a patient to look to the side.
Clinical: Because of its long intracranial course, CN VI is the most frequently injured cranial nerve in the setting of raised intracranial pressure — it is compressed as it bends over the petrous apex. A unilateral CN VI palsy causing medial deviation of the eye at rest is a classic “falsely localizing sign” that suggests raised ICP rather than a primary CN VI lesion. In veterinary neurology, inability to abduct the eye is tested as part of the vestibulo-ocular reflex (physiologic nystagmus / oculocephalic reflex). Failure of the eye to move laterally when the head is moved is a CN VI sign.
Memory trick: Abducens ABducts. VI = six = lateral. Damage = eye turns inward (the lateral rectus can’t pull it out). Most commonly injured CN with raised ICP because of its long route.
VII
Both
Facial — Facial expression, taste, and the nerve behind Bell’s palsy
Anatomy: CN VII is one of the most functionally complex cranial nerves. Its motor fibers arise from the facial nucleus in the pons and supply all muscles of facial expression. Its special sensory fibers (taste) come from the geniculate ganglion and supply the anterior two-thirds of the tongue via the chorda tympani. Its parasympathetic fibers supply the lacrimal gland (via the greater petrosal nerve to the pterygopalatine ganglion) and the submandibular and sublingual salivary glands (via the chorda tympani to the submandibular ganglion). The nerve passes through the internal auditory canal, the facial canal within the temporal bone, and exits the skull at the stylomastoid foramen. Within the parotid gland, it divides into temporal, zygomatic, buccal, marginal mandibular, and cervical branches.
Clinical: Bell’s palsy is the most common cause of unilateral facial nerve palsy — an acute, idiopathic lower motor neuron CN VII palsy producing weakness of the entire ipsilateral face including the forehead. This is the key clinical distinction: upper motor neuron (cortical) lesions such as stroke spare the forehead because the forehead muscles receive bilateral cortical innervation. Lower motor neuron lesions take out the entire face. In veterinary medicine, CN VII palsy is extremely common and produces inability to close the eye, drooping of the lip and ear, deviation of the nose, and inability to move the ear. Otitis media/interna is a common cause in dogs and cats due to the nerve’s proximity to the middle ear.
Memory trick: Seven letters in SMILING — CN VII makes you smile. UMN spares forehead, LMN takes out everything. Bell’s palsy = LMN = whole face. Chorda tympani = taste + saliva = through the middle ear.
VIII
Sensory
Vestibulocochlear — Hearing and balance — two systems in one nerve
Anatomy: CN VIII has two distinct functional components. The cochlear division arises from the spiral ganglion of the cochlea and carries auditory information from hair cells in the organ of Corti to the cochlear nuclei in the medulla. The vestibular division arises from the vestibular ganglion and carries information from the semicircular canals (angular acceleration), the utricle, and the saccule (linear acceleration and gravity). Both divisions travel together in the internal auditory canal alongside CN VII before entering the brainstem at the pontomedullary junction. Central processing of vestibular information occurs in the four vestibular nuclei in the medulla and pons, with projections to the cerebellum, spinal cord (vestibulospinal tract), and extraocular nuclei (vestibulo-ocular reflex).
Clinical: Damage to the cochlear division produces sensorineural hearing loss or tinnitus. Damage to the vestibular division produces vertigo, nystagmus (the fast phase is away from the side of the lesion in peripheral vestibular disease), nausea, head tilt, and falling or rolling toward the affected side. The distinction between central and peripheral vestibular disease is one of the most important clinical skills in veterinary neurology. BAER testing (brainstem auditory evoked response) is used routinely in veterinary medicine to assess cochlear and CN VIII function, particularly in Dalmatians and white cats predisposed to congenital deafness.
Memory trick: Eight looks like headphones with two loops. Two components: cochlear (hearing) and vestibular (balance). Head tilt = vestibular. Nystagmus fast phase away from lesion in peripheral disease. BAER = CN VIII.
IX
Both
Glossopharyngeal — Taste and sensation from the posterior tongue and throat
Anatomy: CN IX arises from the medulla and exits the skull through the jugular foramen alongside CN X and XI. It supplies special sensory (taste) and general sensory (pain, temperature, touch) to the posterior one-third of the tongue and the pharynx. Its motor fibers supply the stylopharyngeus muscle (a pharyngeal elevator). Its parasympathetic fibers originate in the inferior salivatory nucleus and supply the parotid gland via the tympanic nerve, lesser petrosal nerve, and otic ganglion. CN IX provides the afferent limb of the gag reflex — sensory input from the posterior pharynx triggers the reflex — while CN X provides the efferent limb.
Clinical: Isolated CN IX lesions are rare because the nerve travels in close proximity to CN X and XI through the jugular foramen, and lesions in this area typically affect all three. Loss of the gag reflex, reduced salivation, and loss of sensation in the posterior pharynx are the key features. CN IX is clinically important in veterinary neurology primarily through its role in swallowing and the gag reflex. Dysphagia in veterinary patients often reflects pathology affecting the combined vagoglossopharyngeal complex rather than CN IX in isolation.
Memory trick: Glosso = tongue. Pharyngeal = throat. Nine = posterior everything (comes after the facial at the front). Gag reflex = IX in, X out.
X
Both
Vagus — The wanderer — the most important nerve you will use in clinical practice
Anatomy: The vagus nerve is the longest cranial nerve, extending from the medulla all the way into the abdomen. It exits the skull through the jugular foramen and descends in the neck within the carotid sheath. In the thorax, the vagus nerves provide parasympathetic innervation to the heart (slowing heart rate via the SA and AV nodes), the lungs (bronchoconstriction and mucus secretion), and the esophagus. In the abdomen, the left vagus becomes the anterior vagal trunk and the right becomes the posterior vagal trunk, supplying parasympathetic innervation to the stomach, small intestine, and proximal large intestine (to the splenic flexure). Motor branches supply the muscles of the soft palate, pharynx, and larynx. The recurrent laryngeal nerves — branches of the vagus — supply all intrinsic laryngeal muscles except the cricothyroid. The right recurrent laryngeal loops around the right subclavian artery; the left loops around the aortic arch, giving it a much longer intrathoracic course and making it more vulnerable to damage from mediastinal masses.
Clinical: Vagal tone is the primary determinant of resting heart rate. Vasovagal syncope occurs when an exaggerated vagal response causes bradycardia and hypotension. Damage to one vagus produces hoarseness (recurrent laryngeal branch), dysphagia, and deviation of the uvula away from the lesion side. Bilateral vagal damage produces severe swallowing and respiratory dysfunction. In veterinary medicine, laryngeal paralysis is one of the most common presentations of vagal or recurrent laryngeal nerve pathology, particularly in large breed dogs (Labrador Retrievers). Megaesophagus is another veterinary manifestation of vagal dysfunction. The vagus also mediates the vasovagal reflex, which is why stimulation of the vagus (carotid massage, ocular pressure) can slow the heart rate — a technique used in veterinary cardiology.
Memory trick: Vagus = vagrant = wanders everywhere. X = 10 = crosses into the abdomen. Damage = hoarse voice + uvula deviation away from lesion. The left recurrent laryngeal loops around the aortic arch (longer = more vulnerable). Vagal tone = heart rate control.
XI
Motor
Accessory — The nerve that shrugs — and turns the head
Anatomy: CN XI has an unusual origin: its spinal roots arise from the anterior horn cells of the upper cervical spinal cord (C1-C5 or C1-C6), ascend through the foramen magnum, join a small cranial root from the medulla, and exit the skull through the jugular foramen. The spinal accessory nerve then supplies the sternocleidomastoid muscle (which turns the head to the contralateral side) and the trapezius muscle (which elevates the shoulder and retracts the scapula). The cranial root joins CN X and supplies some pharyngeal muscles, but is often considered functionally part of the vagus complex.
Clinical: CN XI damage produces weakness of the ipsilateral sternocleidomastoid (difficulty turning the head away from the lesion side) and trapezius (inability to shrug the ipsilateral shoulder, wasting of the trapezius over time). This pattern is seen with jugular foramen lesions, posterior fossa surgery, or neck dissection. In veterinary medicine, CN XI is rarely assessed in isolation but is included in the general assessment of head and neck posture and muscle tone.
Memory trick: Eleven = two parallel lines = two muscles: SCM and trapezius. Shrug = XI. Head turns AWAY from the lesion (SCM turns head contralaterally, so damage = can’t turn head to that side).
XII
Motor
Hypoglossal — The tongue’s nerve — and the one that deviates toward the damage
Anatomy: CN XII arises from the hypoglossal nucleus in the medulla and exits the skull through the hypoglossal canal. It supplies all intrinsic and extrinsic tongue muscles except the palatoglossus (which is supplied by CN X). The genioglossus is the primary tongue protrusor — it pulls the tongue forward and to the opposite side. With bilateral genioglossus action, the tongue protrudes straight. With unilateral damage, the intact genioglossus on the unaffected side pushes the tongue toward the damaged side, so the tongue deviates toward the lesion.
Clinical: Tongue deviation toward the lesion side is the hallmark of a lower motor neuron CN XII lesion. Over time, there will be ipsilateral tongue atrophy and fasciculations. In upper motor neuron lesions (contralateral cortex or corticobulbar tract), the tongue deviates away from the lesion (contralateral weakness), there is no atrophy, and no fasciculations. In veterinary medicine, CN XII is tested by observing tongue movement and symmetry. Inability to retract the tongue, asymmetric tongue movement, or tongue atrophy are all indicators of CN XII pathology. Dysarthria (difficulty forming words) is the human clinical correlate that will be used in NAVLE cases.
Memory trick: Hypo = under. Glossal = tongue. Last nerve = under the tongue last. Tongue deviates TOWARD the lesion (the good side pushes, the weak side can’t resist). No atrophy in UMN, atrophy + fasciculations in LMN.
The Cranial Nerve Examination: What You’re Actually Testing
Understanding the twelve cranial nerves as a list is one thing. Using them as a diagnostic tool is the skill that transforms this knowledge into clinical competence. The cranial nerve examination is one of the first structured assessments you will perform on a neurological patient in clinical rotations, and it remains one of the most informative parts of any neurological evaluation throughout your career.
Here is what each component of the cranial nerve exam is actually testing in a veterinary patient.
THE VETERINARY CRANIAL NERVE EXAM
Menace response: Tests CN II (afferent: sees the threat) and CN VII (efferent: blinks). If menace is absent but PLR is intact, the deficit is in the visual cortex or optic radiations, not the optic nerve itself.
Pupillary light reflex (PLR): Afferent = CN II. Efferent = CN III (parasympathetics). Tests the integrity of the midbrain. A fixed dilated pupil with intact menace suggests CN III damage. Loss of both PLR and menace suggests optic nerve or retinal pathology.
Strabismus and eye position: Tests CN III, IV, VI. Down-and-out at rest = CN III. Failure to abduct = CN VI. Subtle strabismus when looking down-and-in = CN IV. Vestibular strabismus (positional) is also assessed here.
Facial sensation and corneal reflex: Afferent of corneal reflex = CN V1. Efferent = CN VII (blink). Tests trigeminal function. Poke the face lightly — does the patient feel it and respond?
Facial symmetry and movement: Tests CN VII. Lip droop, ear droop, inability to close the eye, asymmetry of the nose, inability to move the ear are all CN VII signs.
Physiologic nystagmus (VOR): Move the head side to side and watch the eyes. Normal = eyes move in the direction opposite to head movement (doll’s eye reflex). Absent VOR = CN VIII or brainstem pathology.
Gag reflex and swallowing: Tests CN IX (afferent) and CN X (efferent). Touch the pharynx lightly. Absent gag + dysphagia = CN IX/X complex pathology.
Tongue movement: Tests CN XII. Watch the tongue protrude. Deviation, atrophy, or fasciculations are CN XII signs.
Lesion Localization: Nerve Damage and Its Clinical Signs
This table is the clinical application of everything above. Know what each nerve does and you can read this table forwards and backwards — given the nerve, know the sign; given the sign, identify the nerve.
Nerve damaged
What you’ll see clinically
CN I (Olfactory)
Anosmia — loss of smell. Often the first sign of traumatic brain injury (shearing of olfactory fila as they pass through the cribriform plate). Also early in neurodegenerative diseases.
CN II (Optic)
Visual field deficits depending on lesion location. Full transection = blindness ipsilateral eye. Optic chiasm = bitemporal hemianopia. Optic tract = contralateral homonymous hemianopia.
CN III (Oculomotor)
Eye deviates laterally and downward (“down and out”). Ptosis (drooping eyelid). Fixed dilated pupil. Complete ptosis + down-and-out gaze = classic CN III palsy.
CN IV (Trochlear)
Diplopia looking down and inward. Patient tilts head away from affected side to compensate. Often missed clinically. Ask patients to look at their feet.
CN V (Trigeminal)
Loss of facial sensation. Weakness of mastication (jaw deviates toward affected side on opening). Loss of corneal reflex (afferent limb). Trigeminal neuralgia = severe episodic facial pain.
CN VI (Abducens)
Eye cannot abduct (turns inward at rest). Horizontal diplopia. Most commonly injured CN with raised ICP due to its long intracranial course.
CN VII (Facial)
Facial droop — all of ipsilateral face if LMN lesion (Bell’s palsy), forehead spared if UMN lesion (stroke). Loss of taste anterior 2/3 tongue. Hyperacusis (stapedius paralysis). Cannot close eye fully.
CN VIII (Vestibulocochlear)
Cochlear: sensorineural hearing loss, tinnitus. Vestibular: vertigo, nystagmus, nausea, disequilibrium. BAER testing evaluates this nerve in veterinary patients.
CN IX (Glossopharyngeal)
Loss of gag reflex (afferent limb). Loss of taste and sensation posterior tongue. Decreased salivation. Rarely injured in isolation.
CN X (Vagus)
Hoarse voice (recurrent laryngeal nerve branch). Dysphagia. Deviation of uvula away from lesion. Bradycardia if bilateral. Loss of cough reflex. Gastroparesis.
CN XI (Accessory)
Weak or absent shoulder shrug on affected side. Inability to turn head away from lesion side. Trapezius wasting visible over time.
CN XII (Hypoglossal)
Tongue deviates TOWARD lesion side (weak side cannot push, strong side pushes tongue across). Tongue atrophy and fasciculations if LMN. No deviation at rest if UMN.
Why This Matters Beyond the Exam
You are going to perform cranial nerve examinations for the rest of your career. Every time a dog comes in with a head tilt, you are assessing CN VIII. Every time a cat has a droopy lip, you are assessing CN VII. Every time a large breed dog presents with a honking cough and exercise intolerance, you are considering the recurrent laryngeal branch of CN X. Every time an animal has trouble swallowing, you are thinking about CN IX and X together.
The cranial nerves are not a memorization exercise that ends when the practical is over. They are the anatomical framework for every neurological examination you will ever conduct. The time you invest in understanding them now — not just memorizing them but understanding what each one does and what its damage produces — pays dividends throughout your clinical years and throughout your career.
Study them until the mnemonic is automatic. Then study them until the clinical signs make sense. Then study them until you can look at a patient and work backward from the sign to the nerve to the lesion location. That last level is what makes you a good clinician. Start working toward it now.
The cranial nerves are not a memorization exercise that ends with the practical. They are the anatomical framework for every neurological examination you will conduct for the rest of your career.
Scrub Squad · Day 3 of 99 · Mind
This article is part of the Scrub Squad 99-day program from Vet Candy. Free for every first-year vet student. Earn your De-Scrub certificate on Day 99.