

Every Kind of Practice Job Type in Veterinary Medicine
Nobody Told You There Were This Many Choices
When most people imagine veterinary practice, they picture one thing: a doctor in a clinic, a dog on the table, a client on the other side. That image is not wrong. It is just wildly incomplete. The reality of veterinary practice in 2026 is that there are more configurations, ownership structures, specialty environments, and career paths than at any point in the history of the profession, and most veterinary professionals make their first career decisions without a complete picture of what is actually available to them.
This is not a small problem. Choosing the wrong practice environment is one of the leading drivers of burnout, career dissatisfaction, and early exits from the profession. Not because the work is wrong, but because the setting is. A veterinarian who is built for the slow, deep relationships of a private rural practice will be miserable in a high-volume corporate urgent care. A veterinarian who is energized by the chaos and complexity of a teaching hospital emergency floor will be quietly bored in a suburban wellness-only clinic. Getting this match right is the whole point of Dream Job Matchmaker, and getting it right requires understanding all of your options first.
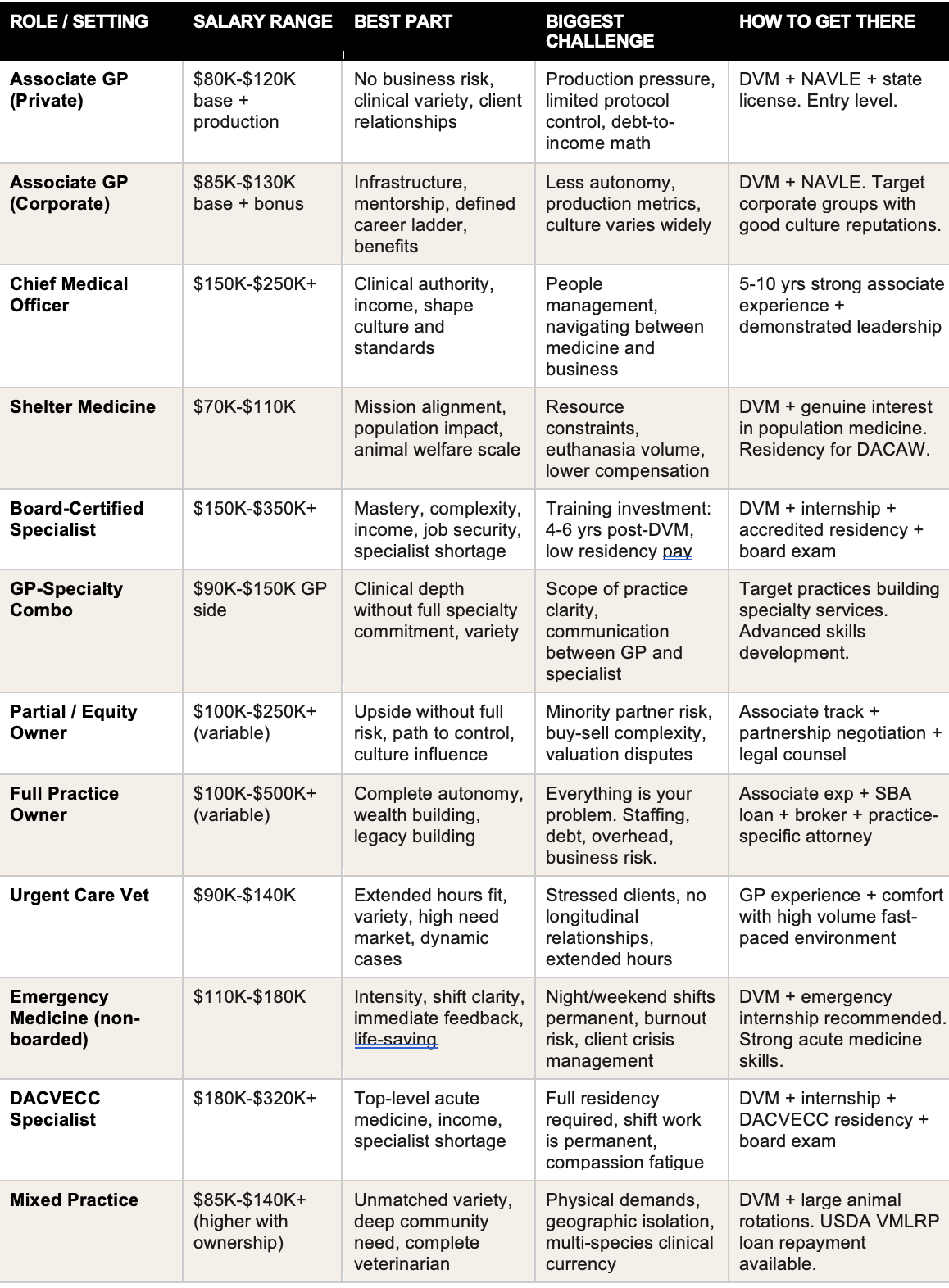
Here is every major practice configuration in veterinary medicine, what it actually looks like from the inside, and what it takes to get there.
The Associate Veterinarian — General Practice
The associate veterinarian in general practice is where the majority of new graduates begin and where most of the profession spends the bulk of its working life. You are employed by a practice, you see appointments, you practice medicine, and at the end of the day you go home. The practice manages the business, the HR, the equipment, the billing, and the overhead. Your job is to be a great clinician.
That sounds simple, and in some ways it is. The associate role is also one of the most emotionally demanding positions in veterinary medicine because you carry the full weight of patient care without the control that ownership provides. You see the cases, you make the recommendations, and then you watch clients make financial decisions that affect outcomes you care deeply about. You manage grief, deliver bad news, and navigate the complexity of human-animal relationships all day, every day, on someone else's schedule.
What it looks like day to day: 15 to 25 appointments depending on practice type. Wellness visits, sick patients, dentistry, soft tissue surgery, in-house diagnostics, client communication, medical record documentation. You are a generalist and you are expected to be excellent across a wide range.
Salary range: $80,000 to $120,000 to start. Production pay models can push this significantly higher. Geographic market and practice type matter enormously.
The best part: Variety, patient relationships, the satisfaction of clinical problem solving, no business responsibility if you do not want it.
The hardest part: Production pressure, emotional labor, limited control over protocols and culture, and the debt-to-income math that makes early-career GP feel financially tight.
How to get there: Graduate from an AVMA-accredited DVM program, pass the NAVLE, obtain state licensure. Associate positions are available immediately post-graduation in most markets.
The reality check
Most veterinarians underestimate how much the practice culture and the ownership philosophy affect their daily experience as an associate. The medicine may be the same from practice to practice. The experience of practicing it is not. Interview the culture as hard as you interview the compensation.
Chief Medical Officer or Medical Director
The Chief Medical Officer or Medical Director is the clinical leadership role of a practice or practice group. It is where clinical expertise meets organizational responsibility, and for many veterinarians it represents the highest-earning configuration available within employed practice without ownership.
This role looks very different depending on the setting. In a single privately owned practice, the Medical Director might spend 60 percent of their time in clinical work and 40 percent in leadership: mentoring associates, developing protocols, managing the relationship between the medical team and ownership. In a corporate group overseeing multiple locations, the clinical work drops and the strategic and administrative work expands significantly.
What it looks like day to day: A mix of clinical work and leadership functions. Hiring and mentoring associates, developing and enforcing clinical standards, managing quality metrics, serving as the liaison between clinical staff and business ownership, handling complex cases that get escalated from associates.
Salary range: $150,000 to $250,000 or more in corporate groups. Bonus structures tied to practice performance are common.
The best part: Significant income, clinical authority, the ability to shape culture and clinical standards, and a career path that does not require the financial risk of ownership.
The hardest part: People management is hard. You are managing veterinarians who went to school for eight years and have strong opinions. Conflict resolution, performance management, and coaching under production pressure are daily realities that nobody prepares you for.
How to get there: Typically requires 5 to 10 years of strong associate performance with demonstrated leadership ability. Some veterinarians pursue an MBA or veterinary leadership certificate program. Corporate groups actively recruit experienced clinicians. Being known in your market and visible in your professional community accelerates the path.
Shelter Medicine
Shelter medicine is one of the most underrepresented and misunderstood career paths in veterinary education, and it is also one of the most mission-driven practices available. Veterinarians who work in shelter medicine are practicing population health in addition to individual patient care, operating within resource constraints that would be unimaginable in private practice, and doing work that has a direct and measurable impact on animal welfare at scale.
Shelter medicine has evolved significantly in the past two decades. Modern shelters are not the depressing facilities of an earlier era. Many are sophisticated organizations with real budgets, experienced teams, progressive medical protocols, and a genuine culture of continuous improvement around animal outcomes. Board certification in shelter medicine through the American College of Animal Welfare is a relatively new specialty designation that reflects how far the field has matured.
What it looks like day to day: High volume intake exams, population disease management, surgical sterilization at volume, vaccination programs, individual patient care for treatable conditions, euthanasia decisions made using established criteria, staff and volunteer training, community outreach.
Salary range: $70,000 to $110,000 at most shelters. Municipal positions include government benefits. Academic shelter medicine positions at veterinary schools pay on the academic salary scale.
The best part: Mission alignment, measurable community impact, population medicine expertise that is unique and increasingly valued, and the knowledge that your work is saving lives at scale rather than one at a time.
The hardest part: Resource constraints are constant. Euthanasia volume, even in progressive shelters, is a reality that requires genuine psychological resilience. Compensation lags significantly behind private practice. The emotional weight is real and has to be managed actively.
How to get there: Graduate DVM plus genuine interest in population medicine and animal welfare. A shelter medicine residency program leads to DACAW board certification. Many shelter veterinarians move into the field directly from general practice. Volunteering or rotating through a shelter during school significantly accelerates the path.
The compensation reality
Shelter medicine veterinarians are among the most dedicated professionals in the field and among the most underpaid. This is a known equity problem in veterinary medicine and one that advocacy organizations are actively working to address. If salary is a primary driver, shelter medicine requires a genuine value alignment conversation with yourself before committing.
Board-Certified Specialist
Becoming a board-certified veterinary specialist is the longest, most demanding, and for the right veterinarian, most rewarding path in the profession. It requires completing an accredited internship, then a multi-year residency program, meeting extensive case and publication requirements, and passing a rigorous specialty board examination. The process takes 4 to 6 years post-DVM for most specialties and involves residency salaries that are far below what a general practitioner earns during the same period.
The specialists who thrive are not the ones who pursued it for the income, although the income is real and significant. They are the ones who cannot imagine spending their career as a generalist, who are genuinely energized by complexity, and who want to be excellent in one specific discipline rather than competent across all of them.
Common specialties: Surgery (DACVS), Emergency and Critical Care (DACVECC), Internal Medicine (DACVIM), Dermatology (DACVD), Cardiology (DACVIM-Cardiology), Neurology (DACVIM-Neurology), Oncology (DACVIM-Oncology), Ophthalmology (DACVO), Radiology (DACVR), Anesthesia (DACVAA), Dentistry (DAVDC), Exotic Animal Medicine (DACZM).
Salary range: $150,000 to $350,000 or more depending on specialty and market. Surgery and Emergency and Critical Care tend to be at the higher end. Production-based compensation at busy referral hospitals can push earnings significantly above base.
The best part: Mastery of a specific discipline, complex and intellectually stimulating cases, the satisfaction of being the person other veterinarians call when they are stuck, high income, and exceptional job security due to perpetual specialist shortage.
The hardest part: The training investment is enormous in both time and foregone income. Residency pay is low. The board exam is genuinely difficult. Some specialties, particularly Emergency and Critical Care, involve permanent shift work including nights and weekends.
How to get there: DVM, then internship (strongly recommended for most specialties), then an accredited residency program, then board examination. The residency application process is competitive and requires strategic planning starting in the third year of veterinary school.
General Practice with In-House Specialty Services
An increasingly common configuration is the general practice that has expanded to include one or more specialty services in-house, whether through hiring a boarded specialist on staff, establishing a specialist referral day where a specialist comes to the practice, or building a hybrid model where the GP veterinarians develop advanced skills in a specific area without pursuing full board certification.
This model benefits both the practice and the clients. Practices that offer in-house specialty consultations or procedures retain cases they would otherwise refer out, increasing revenue and client satisfaction. Clients receive specialist-level care without the referral hospital overhead or wait time.
What it looks like day to day: Varies significantly by how the specialty service is structured. A GP with in-house ultrasound and a visiting cardiologist twice a month looks very different from a hybrid practice with a full-time internist on staff. The GP-specialist combo model requires strong communication between the general practitioners and the specialist to manage cases and client expectations effectively.
Salary range: GP associate salaries with potential for higher production if the practice captures specialty-level case revenue. Specialists working within a GP practice are typically compensated on the specialist salary scale.
The best part: Variety and clinical depth without the full commitment of a specialty hospital. GPs in these settings develop skills and case exposure that pure general practitioners rarely encounter.
The hardest part: Scope of practice clarity is essential. Without clear protocols about what the GP handles versus what goes to the specialist, cases can fall through the gaps and client communication can become inconsistent.
How to get there: As a GP, target practices that have established or are building specialty service lines. As a specialist, this model offers more lifestyle flexibility than a traditional referral hospital and an opportunity to build a different kind of practice relationship.
Privately Owned Practice vs. Corporate Group Practice
This is the conversation that dominates veterinary professional discourse right now and it generates more heat than it probably deserves. The private versus corporate question is not a question of good versus evil. It is a question of what environment best fits your professional values, your career goals, and your tolerance for different kinds of tradeoffs.
Privately Owned Practice
A privately owned practice is owned by one or more veterinarians who are typically also practicing clinicians. The owner or owners set the culture, the clinical standards, the fee structures, and the practice philosophy. Associates in privately owned practices often have more direct access to ownership, more flexibility in clinical protocols, and a stronger sense of community within the practice. They may also have less infrastructure support, fewer formal mentorship programs, and more variable compensation packages than corporate counterparts.
Corporate Group Practice
Corporate veterinary groups, including Mars Veterinary Health, National Veterinary Associates, VCA, Blue Pearl, Ethos, and others, now own a substantial and growing percentage of veterinary practices in the United States. Corporate practice offers standardized protocols, established HR infrastructure, mentorship programs, competitive benefits packages, and defined career ladders that private practice rarely provides. The tradeoffs include less clinical autonomy, production metrics that can feel disconnected from patient care values, and a culture that varies enormously from one corporate group to another.
The honest bottom line: The best private practices are exceptional. The worst private practices are unsustainable. The best corporate practices offer genuine career support and competitive compensation. The worst corporate practices are production mills. The corporate or private label does not tell you which you are walking into. The culture of the specific practice does.
What to ask in every interview regardless of ownership type
What does your associate turnover look like over the past three years and why did people leave? What is the philosophy around production pay and how is it communicated to associates? How are clinical disagreements between associates and ownership handled? These questions will tell you more about the practice than any ownership structure label.
Equity, Partial Ownership, and Full Ownership
Ownership exists on a spectrum, and understanding where you want to land on that spectrum is one of the most important career decisions a veterinarian can make. The distinction between having your name on the door and having meaningful economic ownership in a profitable practice is significant, and the details of buy-sell agreements, valuation methodology, and equity structure matter enormously before you sign anything.
Equity Partnership or Partial Ownership
Many practices offer associate veterinarians a path to partial ownership over time. This can mean buying a minority stake at a fixed price, earning equity through sweat equity arrangements, or being offered a partnership interest in exchange for long-term commitment. The appeal is access to the upside of ownership without the full burden of a controlling interest. The risk is being a minority partner in a practice where the majority owner makes decisions you have no power to change.
Key questions for any partial ownership conversation: How is the practice valued and who controls that valuation? What are the terms of the buy-sell agreement if the partnership dissolves? What decision-making authority does your ownership stake actually carry? What is the path to majority ownership if you want it?
Full Practice Ownership
Full ownership means you carry the full financial risk and the full reward. You make every decision about culture, compensation, protocols, staffing, and the direction of the business. Buying an existing practice typically involves an SBA loan, a down payment of roughly ten percent of the purchase price, and inheriting an existing client base, team, and equipment. Building from scratch means zero inherited clients but complete control over what you build.
Salary range: Highly variable. A practice owner in the first few years of owning a struggling or newly purchased practice may earn less than an associate. An established owner in a productive practice can earn $200,000 to $500,000 or more. The equity value of the practice itself, which grows over time and is realized upon sale, is where the real wealth building happens.
The best part: Complete autonomy, the ability to build a culture and a clinical environment exactly as you envision it, and the wealth-building potential of equity appreciation.
The hardest part: Everything the business does is your problem. Staffing, equipment failure, billing disputes, client complaints, associate performance issues, regulatory compliance, and the constant weight of overhead and debt.
How to get there: Work as an associate and learn the business. Save aggressively or build a partnership with a financial backer. Engage a veterinary practice broker. Get pre-qualified for an SBA loan. Have a veterinary practice-specific attorney review every document before signing.
Urgent Care
Veterinary urgent care is a relatively new and rapidly growing practice model that fills the gap between general practice and emergency medicine. Urgent care practices typically operate on extended hours, including evenings and weekends, and handle cases that are too urgent to wait for a regular appointment but not acute enough to require a full emergency hospital. Think urinary blockage, lacerations, vomiting that started today, a dog that ate something suspicious.
The urgent care model has grown explosively because it addresses a genuine access problem. Most GP practices are fully booked and cannot accommodate sick patients on short notice. Most emergency hospitals are overwhelmed with true emergencies and the wait times for non-critical urgent cases have become unsustainable. Urgent care fills that middle ground.
What it looks like day to day: Walk-in or same-day appointment model with extended hours. Higher acuity than typical GP wellness visits but lower than true emergency medicine. Fast-paced, high volume, diagnostic and stabilization focused. Cases are often discharged or transferred to the client's regular veterinarian for follow-up.
Salary range: $90,000 to $140,000. Extended hours and weekend shifts often carry premium pay.
The best part: Variety, fast pace, extended hours that suit veterinarians who prefer evenings and weekends, and the satisfaction of being the practice that says yes when the client's regular veterinarian cannot see them.
The hardest part: Urgent care sees a higher proportion of anxious, stressed clients than routine GP practice. Managing client expectations, working without a longitudinal relationship with the patient, and the physical demands of extended hours are real challenges.
How to get there: GP experience plus comfort with a fast-paced, high-volume environment. Urgent care is growing fastest in suburban markets and the hiring need is strong.
Emergency and Critical Care
Emergency veterinary medicine is the specialty of the 3 AM call, the hit-by-car, the acute toxin ingestion, the respiratory failure that walked in three minutes before closing. It is high stakes, high intensity, and for the right veterinarian, completely electric. Emergency medicine is the setting where being fast and being right simultaneously matter more than anywhere else in the profession.
Emergency and Critical Care as a specialty (DACVECC) requires a full residency and board examination. But emergency medicine is also practiced by general practitioners who work in emergency hospitals without board certification, and this represents a large and important segment of the emergency veterinary workforce.
What it looks like day to day: Shift work in a 24-hour emergency hospital. Triaging incoming patients, stabilizing critical cases, performing emergency diagnostics and procedures, communicating with clients who are often in crisis, handing off to the next shift. The pace is relentless and the emotional weight is significant.
Salary range: $110,000 to $180,000 for non-boarded emergency practitioners. $180,000 to $320,000 or more for DACVECC specialists. Night and weekend differential pay is common.
The best part: Adrenaline, clinical intensity, immediate feedback, shift-based schedule that is defined and finite, and the satisfaction of saving lives in acute situations.
The hardest part: Night shifts, weekend work, and holidays are permanent features of this career. Compassion fatigue and burnout are documented at higher rates in emergency medicine than almost any other veterinary setting. The emotional labor of managing clients in crisis is different in character from GP grief and requires specific coping strategies.
How to get there: DVM plus comfort with high-stakes acute medicine. Many emergency veterinarians begin as GP associates and transition. DACVECC board certification requires internship plus residency. An emergency internship accelerates the clinical skill development significantly.
Mixed Practice
Mixed practice veterinarians handle both small and large animal cases, typically in rural or semi-rural markets where the client base includes both family pets and working animals. This is the broadest clinical role in veterinary medicine and the one that requires the most adaptable, resourceful practitioner.
Mixed practice has declined as a percentage of overall veterinary employment as specialization has increased and as urban and suburban markets have grown relative to rural ones. But in agricultural communities across the Midwest, Mountain West, Southeast, and Great Plains, mixed practice is not a historical artifact. It is the backbone of veterinary access and it is desperately underserved.
What it looks like day to day: Morning: a dog dental and a cat wellness visit at the clinic. Afternoon: a farm call for a calving cow and a lameness evaluation on a quarter horse. Evening: emergency call for a colicky horse. The variety is unmatched. The physical demands are real.
Salary range: $85,000 to $140,000, with ownership potential in productive rural markets reaching $180,000 to $260,000.
The best part: Variety that no other practice configuration can match, genuine community need, deep relationships with agricultural families, and the professional satisfaction of being a complete veterinarian.
The hardest part: Physical demands, geographic isolation, the expectation of availability that rural agricultural clients hold for their veterinarian, and the challenge of maintaining clinical currency across species when caseload naturally leans toward one or the other by season.
How to get there: DVM with strong large animal clinical rotations. Many veterinary schools offer rural practice tracks or externship programs with mixed practices. The USDA Veterinary Medicine Loan Repayment Program pays up to $25,000 per year in loan repayment for a three-year commitment to a rural shortage area.
WHAT PRACTICE TYPE IS RIGHT FOR YOU?
This quiz is designed to cut through the noise and tell you which practice configuration actually fits how you are wired. Answer based on how you genuinely feel, not how you think a serious veterinarian should feel. Twelve questions, straightforward scoring.
Scoring: each answer awards points toward one or more practice types. Use the key at the end. Add up your points per category and read the result with the highest total.
Score categories: GP-A = GP Associate, CMO = Medical Director/CMO, SH = Shelter Medicine, SP = Specialist, UC = Urgent Care, ER = Emergency Medicine, OWN = Practice Owner, MX = Mixed Practice
QUESTIONS
Q1. After a long clinical day, the thing that would bother you most is:
A. Not having control over how cases are managed (OWN+2, CMO+2)
B. Never going deep enough on complex cases (SP+2, ER+1)
C. Not feeling like you made a real difference in the community (SH+2, MX+2)
D. Having to deal with business and management issues or slow pace (UC+2, ER+2, GP-A+2, SP+1)
Q2. Your honest relationship with nights, weekends, and on-call:
A. I accept it as part of veterinary medicine (ER+2, MX+2)
B. I’m willing to do some but need predictability (UC+2, GP-A+1)
C. I want a defined daytime schedule as much as possible (SH+2, CMO+1, OWN+1)
D. I will do nights if compensation makes it worth it (ER+2, SP+1)
Q3. When you picture your ideal patient population:
A. A mix of species and cases I could never fully predict (MX+3)
B. Complex, referred cases others cannot solve (SP+3)
C. Animals in need who might not have other options (SH+3)
D. Sick and urgent cases where speed and skill matter immediately (ER+3, UC+2)
Q4. The idea of being responsible for the business side of a practice:
A. Excites me; I want to build something (OWN+3)
B. I would accept it with the right support and upside (OWN+1, CMO+1)
C. I would do it at the leadership level but not full ownership (CMO+3)
D. I actively want to avoid it and focus purely on medicine (SP+2, GP-A+2, SH+1, ER+1)
Q5. Your income goal for the first decade of your career:
A. $80K–$110K if the work is meaningful (SH+2, MX+1, GP-A+1)
B. $120K–$160K for forward momentum (GP-A+1, UC+2, CMO+1)
C. $180K+; willing to invest years of training (SP+3)
D. I want maximum earning potential and equity (OWN+3)
Q6. You are at your best professionally when:
A. I’m indispensable to my community (MX+3, SH+2)
B. I make decisions and drive direction (OWN+3, CMO+2)
C. I am the smartest person in my area of expertise (SP+3)
D. Things are fast-paced and I stay calm (ER+3, UC+2)
Q7. How do you feel about 4–6 more years of training after your DVM:
A. No, I am done training and ready to practice (GP-A+2, UC+2, SH+1)
B. Worth it if the payoff in income and satisfaction is significant (SP+3)
C. I would consider a short structured program but not a full residency (CMO+1, SH+1)
D. I love the academic/training environment and could stay in it (SP+2)
Q8. Your ideal practice culture:
A. One I built myself from scratch (OWN+3)
B. One where I set the standards and guide others (CMO+3)
C. Mission-driven and community-focused (SH+3)
D. Fast, focused, high performance with everyone aligned (ER+2, SP+2)
Q9. When a case exceeds your skill level:
A. I refer confidently and value the specialist relationship (GP-A+2, OWN+1)
B. I want to be the expert others call (SP+3)
C. I figure it out because I may be the only option (MX+3, SH+2)
D. I stabilize and transfer appropriately (ER+3, UC+2)
Q10. The work schedule that genuinely appeals to you:
A. Standard daytime hours at a chosen practice (GP-A+2, SH+2)
B. Shift-based with defined start/end times, no on-call (ER+2, UC+2)
C. My own schedule because I am the owner (OWN+3)
D. Extended hours in urgent care/ER settings (UC+3)
Q11. Where you want to live:
A. Rural or semi-rural, needed by the community (MX+3, SH+1)
B. Urban/suburban, access to resources and opportunities (ER+2, SP+2, GP-A+1)
C. Anywhere, flexible if the opportunity is right (CMO+1, OWN+1, UC+1)
D. N/A (Removed to fit four options per question)
Q12. In twenty years, you want to be known as:
A. The veterinarian this practice and clients built their lives around (GP-A+2, OWN+2)
B. The person who built something lasting and ran it well (OWN+3)
C. The best in the country at my specialty (SP+3)
D. The veterinarian who never turned an animal away or saved lives at 2 AM (SH+3, MX+2, ER+3)
Find the category where you scored highest. If two categories are close, read both. The right answer is often a hybrid or a transition path between two configurations.
YOUR RESULT
GP Associate
You want to practice medicine without carrying the business.
You are wired for clinical work. The exam room, the diagnostic puzzle, the client relationship, the satisfaction of catching something early and getting it right, these are what energize you. You are not indifferent to income or career growth, but the business side of veterinary practice is not where your head is. You want to show up, do excellent medicine, and leave the overhead to someone else. That is a completely legitimate and sustainable career choice, and in the right practice it is an exceptionally good one. The key variable is finding the practice culture and the ownership philosophy that matches yours, because the associate experience is shaped more by where you work than what you do.
Salary range: $80,000 to $130,000 base salary with production potential. Geographic market and practice type significantly affect the ceiling.
Best part: Clinical variety, no business responsibility, the longitudinal relationships with clients and patients, and the consistent demand for skilled general practitioners in virtually every market in the country.
Biggest challenge: Production pressure, emotional labor of client communication and end of life conversations, limited control over protocols and culture, and the debt-to-income math of early-career GP.
How to get there
Graduate DVM, pass NAVLE, obtain state license. Target practices with strong mentorship cultures and low associate turnover. An internship is not required but can accelerate clinical skill development significantly.
Vet Candy note: The most important thing you can do as an associate is interview the culture as hard as you interview the compensation. Ask about turnover. Ask how clinical disagreements are handled. Ask what the mentorship structure looks like. The medicine may be the same everywhere. The experience of practicing it is not.
YOUR RESULT
Chief Medical Officer or Medical Director
You want to lead from the inside without owning the business.
You are a clinician with a leadership instinct. You want to practice medicine and you want to shape how others practice it. You care about clinical standards, about building strong teams, and about being the person who sets the bar rather than meets it. Full ownership does not appeal to you, or does not appeal to you yet, but neither does being an indefinite associate with no influence over the direction of the practice. The Medical Director or CMO role gives you clinical authority, significant income, and the ability to build culture without carrying the full financial risk of ownership.
Salary range: $150,000 to $250,000 or more in corporate group settings. Performance bonuses tied to practice outcomes are common.
Best part: Clinical authority, a career ladder that rewards leadership, the ability to mentor and develop other veterinarians, and income that reflects your expanded role.
Biggest challenge: People management under production pressure. You are the bridge between clinical reality and business expectations, and those two things do not always align. Conflict resolution, performance management, and navigating organizational politics are daily realities that veterinary school does not prepare you for.
How to get there
Build 5 to 10 years of strong associate performance with visible leadership presence. Volunteer for mentorship roles, clinical protocol development, and team leadership opportunities. Some veterinarians pursue an MBA or veterinary leadership certificate program. Make your leadership interest known to ownership early.
Vet Candy note: The transition from clinician to clinical leader is one of the most underestimated shifts in veterinary medicine. The skills that make you an exceptional clinician, precision, independence, high personal standards, can work against you in leadership if you do not adapt them to a team context. Seek out leadership mentorship specifically, not just clinical mentorship.
YOUR RESULT
Shelter Medicine
You want your work to matter at scale, not just one patient at a time.
You are drawn to the mission before the medicine. You want to know that your work is contributing to something larger than the individual appointment, that the animals who come through your doors have a better chance because you were there. Shelter medicine is population health in practice, and it requires a specific combination of clinical competence, psychological resilience, resourcefulness under constraint, and genuine value alignment with animal welfare as a guiding professional principle. The veterinarians who thrive here are not the ones who could not get another job. They are the ones who actively chose this because nothing else felt like it mattered enough.
Salary range: $70,000 to $110,000 at most shelter and humane society positions. Academic shelter medicine faculty positions follow the academic salary scale. Municipal shelter positions often include government benefits and pension.
Best part: Mission alignment that few other settings can match, measurable community impact, population medicine expertise that is increasingly valued in public health and One Health contexts, and the knowledge that your decisions affect thousands of animals rather than dozens.
Biggest challenge: Resource constraints are constant and euthanasia volume is a reality even in the most progressive shelters. The emotional weight requires active management strategies and a strong peer support network. Compensation significantly lags private practice.
How to get there
DVM plus genuine interest in population medicine and animal welfare. The American College of Animal Welfare (ACAW) offers board certification through an accredited shelter medicine residency. Many shelter veterinarians move into the field directly from general practice. Rotate through a shelter program during veterinary school if it is available.
Vet Candy note: Shelter medicine is not the fallback. It is the calling. The veterinarians who treat it like a fallback rarely last. The ones who treat it like the calling it is build careers of extraordinary purpose and professional satisfaction.
YOUR RESULT
Board-Certified Specialist
You want to be the best in the world at one specific thing.
You are not built for generalism. The idea of spending your career being competent across everything and expert in nothing does not satisfy you. You want depth. You want to be the person other veterinarians call when they are stuck. You want to practice at the frontier of what is possible in your specific discipline and to contribute to advancing that frontier. The training investment is real and significant, and you are okay with that because the alternative, a career that does not fully use what you are capable of, is not okay with you.
Salary range: $150,000 to $350,000 or more depending on specialty and market. Surgery, Emergency and Critical Care, and Dermatology tend to anchor the high end of the spectrum.
Best part: Mastery of a specific discipline, the intellectual satisfaction of complex case work, exceptional income and job security given perpetual specialist shortages, and the respect of being the person who holds the knowledge that others depend on.
Biggest challenge: The training pathway is 4 to 6 years post-DVM with below-market residency salaries during that period. The board examination is genuinely difficult. Some specialties require permanent shift work. The opportunity cost of the training years is real and must be planned for.
How to get there
Begin planning in year three of veterinary school. A strong clinical record, faculty relationships, and research or case report contributions improve residency application competitiveness. Internship is strongly recommended and required for most specialties. Identify your target specialty early and build your application around it.
Vet Candy note: The veterinarians who struggle through residency are often the ones who chose their specialty for the income rather than the subject matter. Choose the specialty you would be excited to read about on a Saturday morning, not the one with the highest salary ceiling.
YOUR RESULT
Urgent Care Veterinarian
You want to be the practice that says yes when everyone else is booked.
You like being needed right now. Not next Tuesday at 2 PM, but today, this afternoon, when the dog stopped eating and the owner is panicking and the regular vet cannot get them in for a week. You are energized by cases that come in unplanned, by the diagnostic puzzle of the sick walk-in, and by the satisfaction of stabilizing a patient and sending them home the same day. You want a schedule with defined hours, including evenings and weekends, that match how you actually like to work, and you want a practice environment that values speed, accessibility, and clinical skill in equal measure.
Salary range: $90,000 to $140,000 with premium pay common for extended hours and weekend shifts.
Best part: Variety, a high-need market where your presence genuinely matters, a schedule that works for night owls and weekend workers, and the satisfaction of being the practice that actually got them in.
Biggest challenge: Clients presenting to urgent care are often stressed and sometimes hostile because they have already been turned away elsewhere. Managing expectations without longitudinal client relationships is a specific skill that requires intentional development.
How to get there
Strong GP experience plus comfort with a fast-paced, high-volume diagnostic environment. Urgent care is growing fastest in suburban markets and corporate urgent care groups are hiring aggressively. An emergency internship strengthens the skill set significantly.
Vet Candy note: Urgent care is one of the fastest-growing segments of the veterinary market right now. The veterinarian who gets in early in a growing urgent care market has both strong income potential and an excellent platform for eventual ownership or partnership.
YOUR RESULT
Emergency Medicine Veterinarian
You are built for the cases nobody else wants to see at 2 AM.
You are at your best when the stakes are highest and the clock is running. The acute crisis, the animal who walked in barely alive, the diagnostic sprint that requires you to think fast and act faster, this is where you come alive professionally in a way that a scheduled wellness appointment simply cannot replicate. You accept that nights and weekends are part of the permanent structure of this career because the alternative, a slower pace in a lower-stakes environment, is not where you are most useful or most satisfied.
Salary range: $110,000 to $180,000 for non-boarded emergency practitioners. $180,000 to $320,000 or more for DACVECC board-certified specialists. Night and weekend differential pay is standard.
Best part: The intensity and immediate feedback of emergency medicine are unlike anything else in the profession. Shift-based scheduling provides a clarity of work-life separation that many GPs never achieve. The income is strong. The skill set is exceptional.
Biggest challenge: Compassion fatigue and burnout are documented at higher rates in emergency medicine than almost any other veterinary setting. Night shift health impacts are real and cumulative. Managing clients in acute crisis is emotionally demanding in a specific and relentless way.
How to get there
DVM plus an emergency or rotating internship strongly recommended. DACVECC board certification requires a full residency and board examination. Many emergency veterinarians begin as GPs and transition with intentional skill development and emergency shift exposure.
Vet Candy note: Emergency medicine veterinarians who last in the specialty long-term are the ones who build sustainable self-care practices from day one, not when they finally burn out. Sleep hygiene, psychological support, and deliberate decompression are not optional. Build them in before you need them.
YOUR RESULT
Practice Owner
You are not here to work in someone else's dream. You are here to build your own.
Ownership is not for everyone and it is exactly right for you. You want control of the culture, the clinical standards, the client experience, and the financial structure of your practice. You are willing to carry the weight of the business because the alternative, practicing excellent medicine inside constraints you did not set and cannot change, is genuinely unsatisfying to you. The risk is real. The reward is real. And the sense of building something that is yours in every meaningful way is worth both.
Salary range: Highly variable. A first-year practice owner may earn less than an associate. An established owner in a productive practice earns $200,000 to $500,000 or more. The equity value of the practice itself, realized upon sale, is where the real wealth building happens.
Best part: Complete autonomy over every dimension of your practice, the wealth-building potential of equity appreciation, the ability to create exactly the culture and clinical environment you believe in, and the legacy of building something that outlasts you.
Biggest challenge: Everything is your problem. Staffing, equipment failure, billing disputes, client complaints, regulatory compliance, associate performance management, and the permanent weight of overhead and debt. The emotional labor of ownership is different in character from clinical emotional labor and many owners are unprepared for it.
How to get there
Work as an associate with intentional attention to the business of the practice, not just the medicine. Save aggressively or identify financial partners. Engage a veterinary practice broker. Get pre-qualified for an SBA loan. Have a veterinary practice-specific attorney review every document. Consider a partial ownership or equity partnership as a transitional step before full ownership.
Vet Candy note: The most common mistake first-time practice owners make is underestimating the working capital needs of the first 12 to 18 months. Have more cash reserve than you think you need. The practice will take longer to reach full revenue than your projections suggest and the overhead does not wait.
YOUR RESULT
Mixed Practice Veterinarian
You want to be the complete veterinarian your community cannot do without.
You are not built for one lane. You want the dog on the table in the morning and the calving cow in the afternoon and the emergency horse call at dusk. You want the kind of practice where your clients are farmers and families and ranchers and pet owners and every one of them depends on you in a different and essential way. Mixed practice is the broadest clinical canvas in veterinary medicine and it is where the most adaptable, resourceful, and genuinely complete veterinarians spend their careers.
Salary range: $85,000 to $140,000 in employed mixed practice. Ownership in a productive rural market can reach $180,000 to $260,000 or more.
Best part: Unmatched clinical variety, the professional satisfaction of being genuinely essential to your community, deep and multigenerational relationships with agricultural families, and the opportunity to be a complete veterinarian in a way that specialization never allows.
Biggest challenge: Physical demands of large animal work are real and accumulate over time. Geographic isolation requires intentional strategies for professional connection and clinical development. The expectation of availability that rural agricultural clients carry for their veterinarian is not always compatible with the work-life balance goals that younger veterinary professionals prioritize.
How to get there
DVM with strong large animal clinical rotations during school. Externships with mixed practices are one of the most valuable things a veterinary student can do if this career is the goal. The USDA Veterinary Medicine Loan Repayment Program offers up to $25,000 per year in loan repayment for a three-year commitment to a designated shortage area, which includes most rural mixed practice markets.
Vet Candy note: Mixed practice is one of the most critically needed configurations in veterinary medicine and one of the most undersupported by veterinary education. The students who self-select into it are often the most motivated, self-reliant, and community-oriented practitioners in the profession. If this is your direction, own it with confidence.