

The Anatomy of the Eye
Every layer, every structure, every clinical implication — plus how the eye differs across every species you will treat
COMPANION VIDEO
Dr. DJ Haessler, board-certified veterinary ophthalmologist and OSU CVM graduate, has recorded a companion video walkthrough of ocular anatomy and the ophthalmological examination for Scrub Squad. Watch it after reading this article. The combination of the written framework and the clinical walkthrough is significantly more effective than either alone.
The Anatomy of the Eye
The eye is one of the most anatomically dense structures in the body relative to its size. In a space roughly equivalent to a marble, the globe contains three distinct tissue layers, six extraocular muscles, a specialized fluid production and drainage system, a neural image-capture surface, and a refractive optical system precise enough to focus light to within micrometers. Understanding it anatomically is the foundation for understanding everything ophthalmology asks you to do clinically.
This article walks through the eye systematically, outside in. The fibrous coat first — the structural outer shell. Then the uveal tract — the vascular and functional middle layer. Then the retina — where light becomes neural signal. Then the adnexa — the lids, the lacrimal system, the orbit. Then species comparisons. Then the most common clinical conditions and how the anatomy explains each one.
Read the eye the way you read any complex structure: outside in, proximal to distal. Structure first, function second, pathology third. The pathology makes sense once the anatomy does.
The Fibrous Coat: The Outer Shell
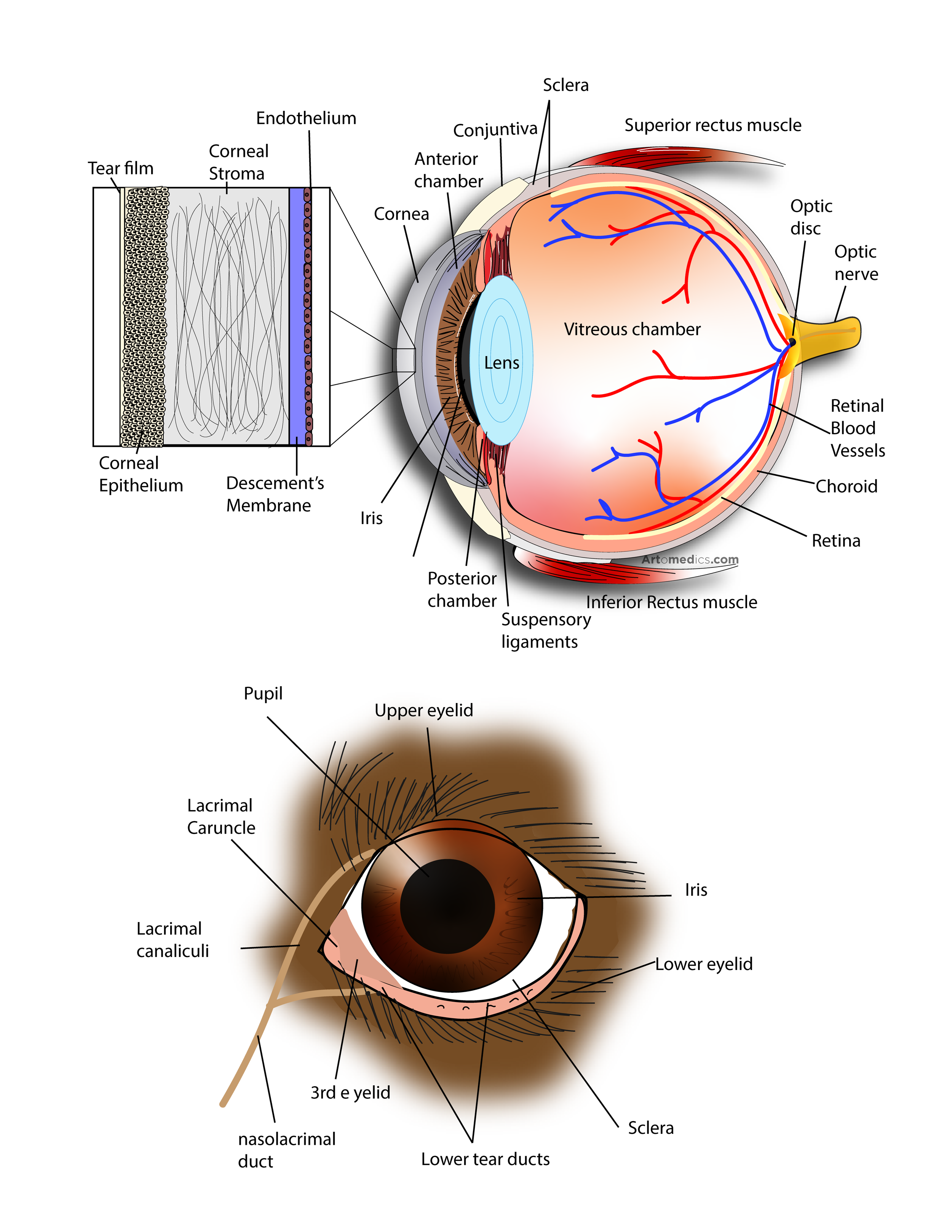
The outermost layer of the globe consists of two structures that together form a continuous protective shell: the sclera and the cornea.
Cornea — Transparent, avascular, highly innervated
Anatomy: The cornea occupies approximately the anterior one-third of the outer coat of the globe. It consists of five layers from outside in: (1) Stratified squamous epithelium (5–7 cell layers, regenerates rapidly — surface cells shed every 7 days, basal cells divide continuously). (2) Bowman's layer (acellular condensation of stroma in some species — present in primates, absent or poorly developed in dogs and cats). (3) Stroma — 90% of corneal thickness, comprised of parallel collagen lamellae with keratocytes between them. The regular arrangement of these lamellae is what makes the cornea transparent. (4) Descemet's membrane — basement membrane of the endothelium, thickens with age. (5) Endothelium — single cell layer that maintains corneal dehydration through active pump function. Endothelial cells cannot regenerate in most domestic species.
Appearance / characteristics: Transparent, dome-shaped, avascular. Receives oxygen directly from the tear film and nutrients from aqueous humor. In most domestic species it is thinner at the center than the periphery (opposite of humans). Normal corneal reflex: V1 (ophthalmic branch of CN V) mediates the afferent sensation; CN VII mediates the efferent blink. Test it at every neurological exam.
Clinical significance: Corneal ulcers: disruption of the epithelial layer. Classified by depth — superficial (epithelium only), deep (into stroma), descemetocoele (only Descemet's and endothelium remain — surgical emergency, will perforate). Fluorescein dye uptake confirms ulceration. Indolent ulcers in Boxers and Corgis fail to heal because the epithelium does not adhere to the stroma. KCS (keratoconjunctivitis sicca / dry eye) — inadequate tear film — is one of the most common causes of corneal disease in dogs.
Pearl: Endothelial cells do not regenerate. Corneal endothelial dystrophy (degeneration of the pump cells) causes progressive corneal edema and cloudiness — most common in Chihuahuas, Boston Terriers, and Dachshunds. Once the endothelium is sufficiently compromised, the cornea remains permanently edematous.
Sclera — Opaque, fibrous, protective
Anatomy: The sclera forms the posterior five-sixths of the outer coat of the globe. It is composed of dense, irregular collagen (unlike the regular parallel arrangement of the corneal stroma — it is the irregular arrangement that makes the sclera white and opaque rather than transparent). The sclera provides the attachment points for the six extraocular muscles and contains the limbus — the transition zone between cornea and sclera where aqueous humor drains and where corneal stem cells reside.
Appearance / characteristics: White and opaque in most species. Thinnest at the insertion sites of the extraocular muscles (a site of predilection for globe rupture in trauma). The episcleral vessels on the surface are visible with magnification and are dilated in conditions of elevated intraocular pressure (glaucoma) or intraocular inflammation (uveitis).
Clinical significance: Scleral injection (redness of the scleral vessels) is a clinical sign of intraocular disease or elevated IOP. Episcleritis — inflammation of the tissue overlying the sclera — is an immune-mediated condition in dogs presenting as raised pink-red masses that can be mistaken for neoplasia. Does not respond to antibiotics. Responds to immunosuppression.
Pearl: The sclera is where the optic nerve exits (optic disc / optic nerve head) — surrounded by a ring of scleral tissue called the lamina cribrosa. Elevated IOP compresses and eventually excavates the lamina cribrosa, damaging the ganglion cell axons that form CN II. This is the mechanism of glaucoma-related blindness.
The Uveal Tract: The Vascular Middle Layer
The uvea is the middle coat of the eye, consisting of three continuous structures: choroid (posterior), ciliary body (middle), and iris (anterior). Together they form the main blood supply to intraocular structures, produce the fluid that fills the eye, and control both pupil size and lens focusing.
Iris — Controls pupil diameter and gives the eye its color
Anatomy: The iris is the most anterior part of the uvea, suspended in the aqueous humor between the cornea and the lens. It contains two smooth muscle groups: the sphincter pupillae (parasympathetically innervated via CN III via the ciliary ganglion — constricts the pupil / miosis) and the dilator pupillae (sympathetically innervated via the long ciliary nerves — dilates the pupil / mydriasis). The stroma of the iris contains the pigment (melanocytes and melanin) that determines eye color.
Appearance / characteristics: In most domestic species the iris is pigmented brown to amber. Blue eyes result from reduced melanocyte density in the stroma (light scatters differently). Heterochromia iridia (different colored irises) is normal in some breeds — common in Australian Shepherds, Dalmatians, Siberian Huskies. Persistent pupillary membranes (PPM) — remnants of the fetal iris vasculature — are common incidental findings.
Clinical significance: Uveitis (inflammation of the uveal tract, often begins with the iris — iritis/anterior uveitis): causes miosis, aqueous flare (protein in aqueous humor, visible with slit lamp), keratic precipitates (white blood cells on corneal endothelium), hypopyon (white cells settling in the anterior chamber), and reduced IOP (ciliary body produces less aqueous when inflamed). Iris melanoma: watch for progressive darkening of an iris lesion in cats — iris melanosis can transform to melanoma. Sequential photography documents progression.
Pearl: The PLR (pupillary light reflex): afferent via CN II, efferent via CN III. Direct PLR = shine light in affected eye, that pupil constricts. Consensual = the other eye also constricts. If direct PLR is absent but consensual is present, the lesion is in CN II (can't carry the afferent signal). If direct is present but consensual absent, the lesion is in CN III of the other eye (can't carry efferent to the other pupil).
Ciliary Body — Produces aqueous humor and controls lens accommodation
Anatomy: The ciliary body is a ring of tissue located posterior to the iris. It has two functional components: the pars plana (smooth posterior part, site of intravitreal injections) and the pars plicata (folded anterior part where aqueous humor is produced by the ciliary processes via active secretion and ultrafiltration). The ciliary muscle — innervated by the parasympathetic system — controls lens shape for accommodation (focusing). Zonular fibers (suspensory ligaments of the lens) run from the ciliary processes to the lens equator.
Appearance / characteristics: Not directly visible on routine examination. The angle at which the ciliary body meets the iris base forms the iridocorneal angle — the drainage angle for aqueous humor. Normal IOP depends on the balance between aqueous production (ciliary body) and aqueous drainage (iridocorneal angle and uveoscleral pathway).
Clinical significance: Glaucoma (elevated IOP) results when drainage is impaired relative to production. Primary glaucoma: drainage angle abnormal from birth (goniodysgenesis — narrow or closed angle). Secondary glaucoma: inflammation, lens luxation, or neoplasia blocking drainage. The carbonic anhydrase inhibitors (dorzolamide, brinzolamide) reduce aqueous production by inhibiting the enzyme needed for active secretion. Beta-blockers (timolol) reduce blood flow to the ciliary body. Both are used in glaucoma management.
Pearl: Lens luxation (subluxation or complete luxation of the lens from its zonular attachments) is a veterinary emergency. Forward luxation of the lens into the anterior chamber blocks aqueous drainage and causes acute glaucoma. Most common in Terriers (genetic predisposition). Signs: trembling of the iris (iridodonesis), abnormal lens position, acute blepharospasm and pain. Treatment: surgical removal of the luxated lens.
Choroid — Primary vascular supply to the outer retina
Anatomy: The choroid is a highly vascular layer between the sclera and the retina that provides oxygen and nutrients to the outer retinal layers (photoreceptors primarily) via diffusion. It is the thickest and most vascular structure in the eye. In many species the choroid contains the tapetum lucidum — a layer of reflective cells (tapetal cells containing zinc-cysteine crystals in dogs; riboflavin in cats) that reflects light back through the photoreceptors to improve low-light sensitivity.
Appearance / characteristics: Not directly visible on fundic examination in most species except as the background glow of the tapetal zone (visible with an ophthalmoscope). The tapetum lucidum appears as the colored, reflective area in the dorsal fundus; the non-tapetal area (where pigment absorbs light) is ventral and darker.
Clinical significance: Hypertensive retinopathy / choroidopathy: systemic hypertension (most common in cats with CKD or hyperthyroidism, dogs with Cushing's disease or renal disease) damages the choroidal vessels, leading to choroidal vasodilation, subretinal fluid accumulation, and retinal detachment. Presenting sign in cats: sudden blindness, widely dilated pupils, with retinal detachment visible on fundic examination.
Pearl: Choroidal hypoplasia: colloquially called 'Collie eye anomaly' — a congenital developmental defect of the choroid most common in Rough and Smooth Collies and related herding breeds. Range from mild (choroidal hypoplasia alone) to severe (staphyloma, retinal detachment, optic disc coloboma). Genetic testing available.
The Retina: Where Light Becomes Neural Signal
The retina is the innermost layer of the globe and the most neurologically complex structure in the eye. It is essentially a displaced piece of brain — it develops from the same neural tube tissue as the CNS and is connected directly to the brain via the optic nerve.
The retina has ten layers, but the key functional ones to know: the retinal pigment epithelium (RPE — the outermost layer, adjacent to the choroid; supports and recycles photoreceptors), the photoreceptor layer (rods and cones), the outer nuclear layer (photoreceptor cell bodies), the inner nuclear layer (bipolar cells, horizontal cells, amacrine cells), the ganglion cell layer (ganglion cell bodies), and the nerve fiber layer (ganglion cell axons, which become CN II).
RODS VS CONES — THE PHOTORECEPTOR COMPARISON
Rods: Extremely sensitive to light (operate in low-light conditions). No color discrimination. Distributed peripherally in the retina. Very numerous in dogs and cats (120+ million in dogs). Responsible for motion detection and night vision. Rods contain rhodopsin (vitamin A-derived photopigment). Rhodopsin bleaches in bright light — this is the basis of the dark adaptation period when you move from bright to dim light.
Cones: Require brighter light. Mediate color vision and fine detail resolution. Concentrated in the area centralis (the fovea equivalent in domestic species — a region of highest cone density for best acuity). Dogs and cats are dichromats (two cone types: blue-sensitive and yellow-sensitive). Humans are trichromats. Birds are tetrachromats and can see UV light. Dogs cannot see red.
Optic disc (optic nerve head): The point where ganglion cell axons exit the eye. No photoreceptors here — it is the physiological blind spot. On fundic examination it appears as a pale oval or round structure in the non-tapetal ventral area of the fundus (in dogs) or more central (in cats). Papilledema (swelling of the optic disc) indicates increased intracranial pressure.
The Adnexa: The Supporting Structures
Eyelids
The eyelids protect the globe, distribute the tear film with blinking, and contain the meibomian glands (tarsal glands) that produce the lipid layer of the tear film. The upper lid in most species is more mobile than the lower. The lid margin (where eyelashes emerge in haired species) and the mucocutaneous junction are important landmarks. Clinical conditions: entropion (inward rolling of the lid margin — causes corneal irritation; common in Chow Chows, Shar Peis, Bulldogs, Rottweilers), ectropion (outward rolling — common in Basset Hounds, Bloodhounds; causes epiphora and conjunctivitis), distichiasis (extra eyelashes from meibomian gland openings — common in Cocker Spaniels, Shih Tzus), and ectopic cilia (cilia emerging from the palpebral conjunctiva — extremely painful corneal irritation).
The Lacrimal System
The lacrimal system produces and drains tears. Tear production comes from three sources: the lacrimal gland (above the lateral canthus), the accessory lacrimal glands (distributed through the conjunctiva), and the nictitans gland (produces approximately 30–40% of the aqueous tear volume in dogs and cats). The tear film has three layers: outer lipid (prevents evaporation, from meibomian glands), middle aqueous (from lacrimal glands), inner mucin (from goblet cells, helps the tear film adhere to the epithelium).
Keratoconjunctivitis sicca (KCS / dry eye) results from insufficient aqueous tear production, most commonly immune-mediated destruction of the lacrimal and nictitans glands in dogs. Signs: mucoid to mucopurulent discharge, dull cornea, corneal pigmentation and vascularization chronically. Diagnosis: Schirmer tear test (normal >15mm/min in dogs). Treatment: cyclosporine or tacrolimus ophthalmic drops (immunosuppressive, prevents further gland destruction and stimulates residual production) plus artificial tears.
The Nictitating Membrane (Third Eyelid)
The third eyelid is a fold of conjunctiva supported by a T-shaped cartilage and containing the nictitans gland at its base. It crosses the eye from the medial canthus and is most prominent in animals with recessed globes. Clinical significance: prolapse of the nictitans gland ('cherry eye') — the nictitans gland pops out of its normal position and appears as a red fleshy mass at the medial canthus. More common in Bulldogs, Beagles, Cocker Spaniels, and other breeds with loose periorbital tissue. Treatment is surgical repositioning (not excision — excising the gland causes KCS). Protrusion of the third eyelid bilaterally ('hoods over the eyes') in cats often indicates pain, illness, or Haw's syndrome.
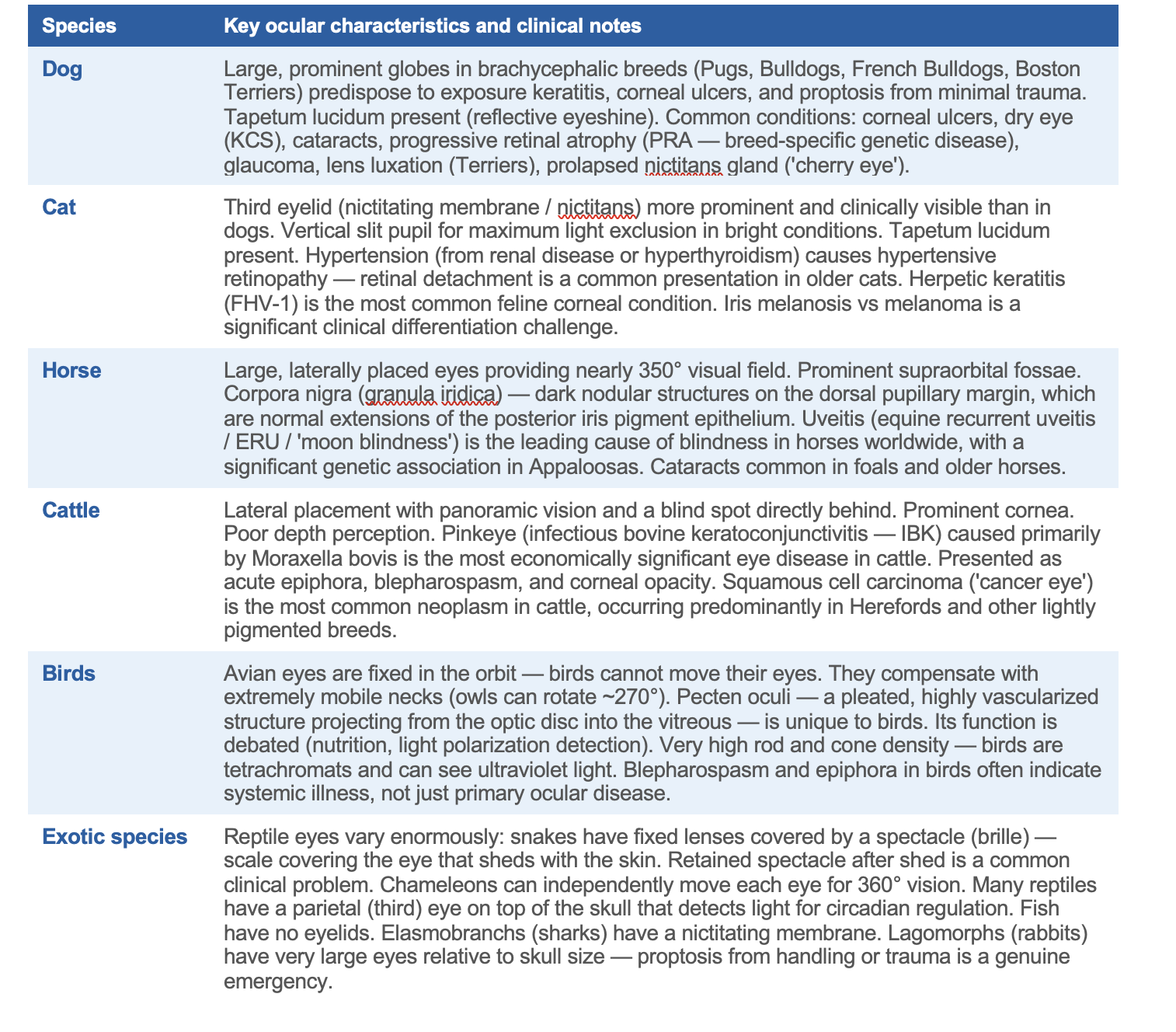
Species-Specific Ocular Anatomy and Common Conditions
The fundamental anatomy described above applies across species, but the specific presentations, common conditions, and clinical approach differ significantly. Knowing these differences before your first ophthalmology rotation prevents the most common errors.
The Ophthalmic Examination: Systematic and Sequential
A complete ophthalmic examination proceeds in order: distant examination (globe position and symmetry, menace response, PLR), adnexal examination (lids, third eyelid, periorbital), conjunctival examination, corneal examination (fluorescein staining, slit lamp if available), anterior chamber assessment (depth, flare, hypopyon, hyphema), iris and lens examination, IOP measurement (tonometry — Tono-Pen or Tonovet; NEVER use a Schiotz tonometer on cats — it produces falsely elevated readings), and fundic examination (direct or indirect ophthalmoscopy, dilate with tropicamide first).
HIGH-YIELD OPHTHALMIC EXAM MNEMONICS
COAG: Cornea — Anterior chamber — Angle (gonioscopy) — Glaucoma screening. The sequence for any patient presenting with a cloudy or red eye.
PLR interpretation: Direct PLR absent + consensual present = CN II lesion ipsilaterally (afferent gone). Direct present + consensual absent = CN III lesion contralaterally (efferent gone to that pupil). Both absent = severe bilateral CN II, brainstem lesion, or pharmacological dilation.
STT < 10mm/min: Definitive KCS. 10–15mm: borderline, treat if clinical signs present. >15mm: normal. Test BEFORE touching the eye or instilling any drops.
Fluorescein rules: Green uptake = ulcer present. No uptake on a dull, irregular cornea = stromal edema (endothelial failure), not ulceration. A descemetocoele will NOT take up fluorescein (Descemet's membrane is hydrophobic), but the surrounding stroma will — look for a clear 'eye' within a staining ring.
Why Ophthalmology Is One of the Most Rewarding Specialties in Veterinary Medicine
The eye is a direct window into the patient's systemic health. Hypertension, diabetes, immune-mediated disease, infectious disease, neoplasia, and neurological conditions all leave signatures in the globe. A thorough fundic examination in a geriatric cat with weight loss may reveal the retinal detachment of hypertension that explains why the cat has been missing the litter box. A careful corneal examination in a Collie puppy may identify the choroidal changes of collie eye anomaly before the owner knows it exists.
Ophthalmology also rewards the student who learns the anatomy in detail, because the examination is entirely anatomy-driven. What you see through the slit lamp maps directly to the layers you have learned here. The fluorescein uptake tells you which corneal layer is disrupted. The IOP tells you whether the drainage system is functional. The fundic image tells you the condition of the choroid, tapetum, and retinal vasculature.
Watch Dr. Haessler's video. It will make every structure in this article come alive in a way that text cannot fully replicate. Then find the ophthalmology room at your school and ask if you can practice with the slit lamp. The eye rewards the student who looks at it with intention.
The eye is a window into systemic health. Hypertension, diabetes, immune disease, neurological lesions — all leave signatures in the fundus, the cornea, or the uvea. Learn the anatomy of the eye and you gain a diagnostic tool that applies to every species and every discipline.
Scrub Squad · Day 7 of 99 · Mind
This article is part of the Scrub Squad 99-day program from Vet Candy. Free for every first-year vet student.