

Blood Cells: The Complete Guide
What every cell does, what it looks like, what its presence or absence means, and why it looks completely different depending on which species you’re examining
Blood is information. Every cell in a blood smear is there for a reason, doing a specific job, and its appearance — or the appearance of cells that shouldn’t be there, or the absence of cells that should be — tells you something precise about what is happening inside the patient in front of you. Learning to read a blood smear is one of the most consistently useful skills in clinical veterinary medicine because it applies to every species and every discipline.
This article covers the complete blood picture: the seven major cell types, their structure, their function, their clinical significance, and the specific abnormalities you will be asked to recognize. It also covers the species-specific variations that trip up first-year students consistently — because what is pathological in a dog may be textbook normal in a horse or a bird, and getting this wrong in a clinical setting has real consequences.
Read this once for orientation. Return to it before your first clinical pathology practical. Stick the species table on your wall.
Learning to read a blood smear is one of the most consistently useful skills in clinical veterinary medicine. Every cell type, every morphological change, every abnormal inclusion tells you something specific. The smear does not lie.
Red Blood Cells (Erythrocytes): The Oxygen Carriers
The erythrocyte has one job: carry oxygen from the lungs to the tissues and return carbon dioxide. It is exquisitely optimized for this function. In mammals, mature RBCs have no nucleus, no mitochondria, and no ribosomes — they have sacrificed the ability to repair themselves and replicate in order to maximize the space available for hemoglobin. A single human RBC contains approximately 280 million hemoglobin molecules.
The biconcave disc shape of mammalian RBCs is not incidental. It increases surface area for gas exchange relative to volume, it allows the cell to deform enough to squeeze through capillaries narrower than its own diameter, and it creates the characteristic central pallor visible on a well-prepared blood smear — the central area where the cell is thinnest and hemoglobin concentration is lowest.
Mammalian RBCs live approximately 60 to 120 days depending on the species (dogs ∼ 110 days, cats ∼ 70 days, horses ∼ 140–150 days). They are produced in the bone marrow from erythroid precursors through a process called erythropoiesis, driven by erythropoietin (EPO) from the kidneys. When they age, they are removed by macrophages in the spleen, liver, and bone marrow.
On a stained smear, normal RBCs are salmon-pink to orange-pink, round, uniform in size (unless there is pathology), and have a pale center that occupies about one third of the cell diameter in dogs and is less prominent in cats.
Bird, reptile, and fish RBCs are nucleated and oval. This is not abnormal. It is how non-mammalian vertebrate RBCs are built. The mammalian anucleate RBC is the evolutionary exception, not the rule.
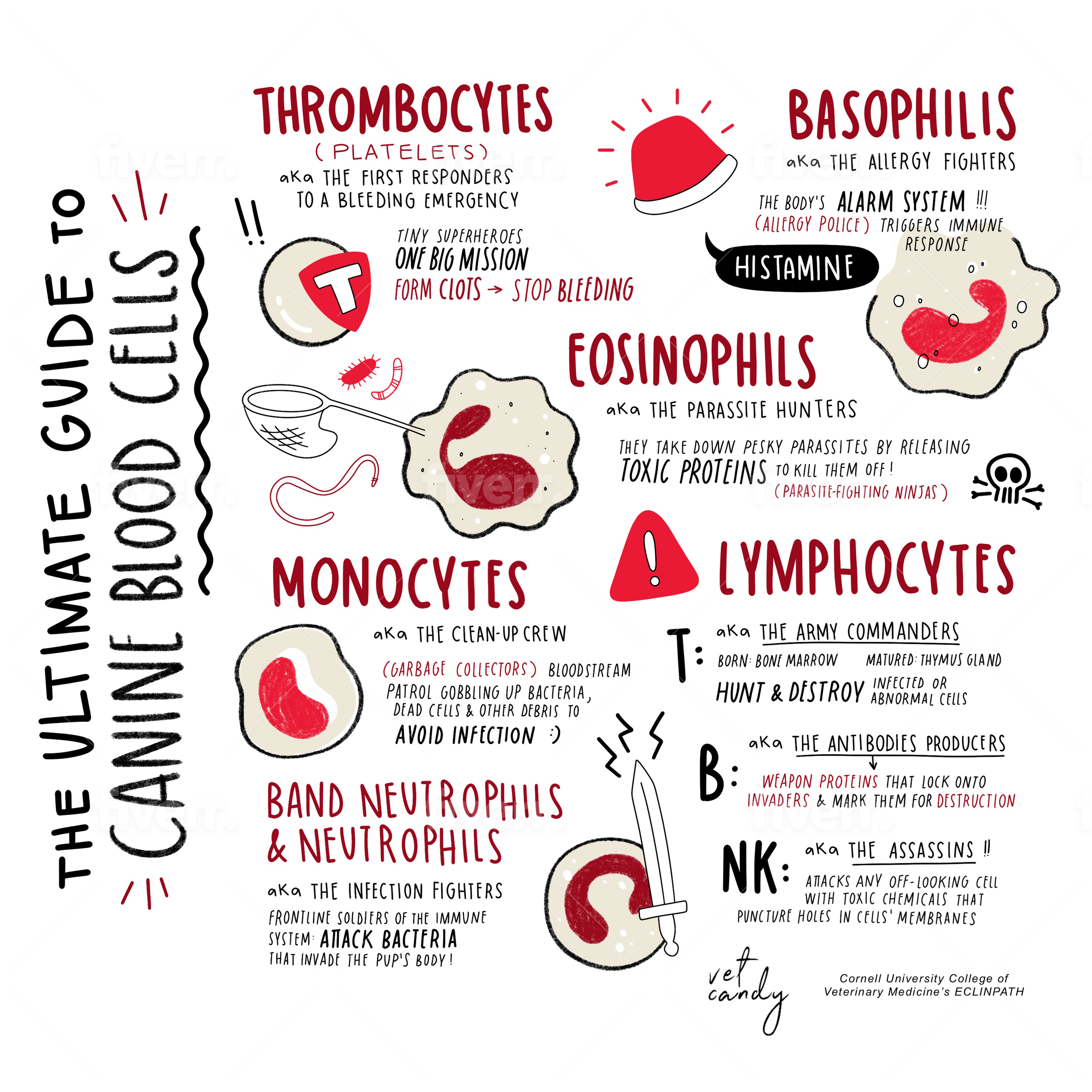
White Blood Cells (Leukocytes): The Immune Sentinels
There are five types of white blood cells, divided into two broad categories: granulocytes (neutrophils, eosinophils, basophils — named for their cytoplasmic granules) and agranulocytes (lymphocytes, monocytes — without visible granules on routine staining). Each has a distinct appearance, a distinct job, and a distinct clinical significance when it is elevated or depleted.
Granulocyte
Neutrophils — The first responders
Structure: Multi-lobed nucleus (2–5 lobes connected by thin strands of chromatin). Pale pink to colorless granules in the cytoplasm. The most abundant WBC in dogs, cats, and humans (50–75% of the differential). Smaller than eosinophils and monocytes.
Function: Primary effectors against bacterial infection. They are recruited rapidly to sites of infection, phagocytose bacteria, and destroy them via oxidative burst and degranulation. Their lifespan in circulation is only 6–12 hours — they migrate into tissues and die at the site of infection.
Clinical pearl: Neutrophilia (increased neutrophils): bacterial infection, inflammation, glucocorticoid administration, physiologic stress. Neutropenia (decreased): overwhelming bacterial infection (consumption exceeds production), bone marrow disease, parvovirus infection. Band neutrophils (horseshoe-shaped, non-segmented nucleus) indicate a left shift — the marrow is releasing immature cells because demand exceeds supply. Toxic changes in neutrophils (Döhle bodies, cytoplasmic vacuolation, toxic granulation) indicate severe systemic inflammation.
Memory trick: Neutrophils = nuclear lobes like a string of purple beads. More lobes = older cell (hypersegmentation seen with glucocorticoids or B12/folate deficiency). Fewer lobes = younger cell, left shift.
Agranulocyte
Lymphocytes — The adaptive immune memory
Structure: Small cell with a large, round, dark purple nucleus that fills most of the cell. Scant pale blue cytoplasm. The smallest WBC. Large granular lymphocytes (LGLs) are a subset with visible azurophilic granules and more cytoplasm.
Function: B lymphocytes differentiate into plasma cells that produce antibodies (humoral immunity). T lymphocytes kill infected cells directly (cytotoxic T cells) or coordinate the immune response (helper T cells). Natural killer (NK) cells destroy abnormal cells without prior sensitization. Lymphocytes circulate, exit into lymph nodes, sample antigens, and re-enter circulation.
Clinical pearl: Most common WBC in cattle, sheep, and pigs (unlike dogs and cats). Lymphocytosis: antigenic stimulation, physiologic (excitement in cats), chronic infection, lymphoma/leukemia. Lymphopenia: acute stress/cortisol release, viral infection, immunosuppression. Reactive lymphocytes (larger, more cytoplasm, deeper blue) indicate active immune stimulation — not the same as neoplastic lymphocytes.
Memory trick: Lymphocytes = small with a large purple nucleus. The nucleus is so big it looks like almost the whole cell. Think of it as a cell that is mostly ‘memory storage’ with very little room for anything else.
Agranulocyte
Monocytes — The bone marrow’s gift to the tissues
Structure: Largest WBC. Kidney-shaped, horseshoe, or amoeboid nucleus — not segmented like neutrophils, not round like lymphocytes. Gray-blue cytoplasm, often with vacuoles (holes). Can look like they have been eating things, which they have.
Function: Monocytes are the circulating precursors to tissue macrophages. They phagocytose debris, dead cells, and pathogens, and present antigens to T cells to activate adaptive immunity. They produce cytokines that orchestrate inflammation. When they enter tissues, they differentiate into macrophages, dendritic cells, or osteoclasts depending on the signals they receive.
Clinical pearl: Monocytosis is associated with chronic inflammation, tissue necrosis, glucocorticoid administration (part of the ‘stress leukogram’: neutrophilia, lymphopenia, monocytosis, eosinopenia), and certain fungal or protozoal infections. Monocytic leukemia is a recognized entity. In dogs, monocytosis following recovery from acute infection signals the cleaning-up phase.
Memory trick: Monocytes = Massive, Moody nucleus (kidney-shaped), gray-blue cytoplasm with vacuoles. They look like they’re always scanning for something to eat. They are.
Granulocyte
Eosinophils — The parasite hunters
Structure: Bilobed nucleus (two lobes, not multi-lobed like neutrophils). The distinguishing feature is the cytoplasmic granules — bright pink-orange in dogs and cats, large and round in horses (some of the most distinctive cells in veterinary hematology), more variable in cattle. Slightly larger than neutrophils.
Function: Eosinophils are recruited to sites of parasitic infection and allergic reactions. They degranulate to release toxic proteins (major basic protein, eosinophil peroxidase) that damage parasites. They also modulate mast cell activity and participate in tissue remodeling. Their cytoplasmic granules are the defining visual feature on any blood smear.
Clinical pearl: Eosinophilia: parasitic infection (think: heartworm, GI parasites, ectoparasites), allergic disease (atopy, asthma), eosinophilic syndromes (eosinophilic granuloma complex in cats, pulmonary infiltrates with eosinophilia in dogs). Always get a fecal and check for parasites before attributing eosinophilia to allergy alone. Eosinopenia is part of the stress leukogram (cortisol suppresses eosinophil release).
Memory trick: Eosinophils = bright ORANGE granules. Think of them as the brightly dressed soldiers sent after parasites. Horse eosinophils have the largest, most distinctive granules of any domestic species — you will not miss them.
Granulocyte
Basophils — The rarest granulocyte
Structure: Bilobed nucleus that is often partially or fully obscured by dark purple to black granules in most species. In cats, basophil granules are pale lavender (easy to confuse with other cells). Often reported as zero on a normal differential count.
Function: Basophils are involved in allergic and hypersensitivity reactions. They degranulate to release histamine, heparin, and other mediators. They are functionally related to mast cells (tissue-resident counterparts) but circulate in the blood in very small numbers. Their exact role is still less completely understood than other WBCs.
Clinical pearl: Basophilia is rare and should always be investigated. Associated with hypersensitivity reactions, heartworm disease (dogs), mast cell tumor (mastocytemia with rare basophilic cells), and some myeloproliferative disorders. In cats, the pale lavender granules make basophils easy to undercount. In birds, basophils have deeply stained granules and are more routinely seen.
Memory trick: Basophils = dark purple-black granules that obscure the nucleus. So dark you can barely see what’s underneath. The cell that does not want to be seen. Found rarely. When you find one, pay attention.
Platelets (Thrombocytes): The Hemostasis Team
Platelets are not true cells — they are anucleate fragments of megakaryocyte cytoplasm that break off into the circulation and live for approximately 8 to 12 days in dogs. They are the smallest formed element in mammalian blood and appear as small, pale lavender to colorless irregular fragments on a blood smear, often clustering at the edges of the slide where the smear thins out.
Their job is primary hemostasis: when vascular endothelium is disrupted, von Willebrand factor bridges the platelet surface receptor (GPIb) to exposed collagen, causing platelet adhesion. Platelets then activate, change shape, and release granule contents (ADP, thromboxane A2, serotonin) that recruit more platelets, forming the primary platelet plug. This plug is then reinforced by the secondary hemostatic cascade (fibrin formation).
A normal platelet count in dogs is approximately 200,000 to 500,000 per microliter. Spontaneous bleeding typically does not occur until counts fall below 20,000 to 30,000. Platelet function can be abnormal even with a normal count (thrombopathia), which is why both count and function assessment matter in bleeding patients.
THE PLATELET CLUMPING TRAP
This is one of the most clinically important artifacts in veterinary hematology, and it catches students and clinicians alike. When blood is drawn with difficulty, handled roughly, or collected in the wrong anticoagulant, platelets can clump together and accumulate at the feathered edge of the blood smear. The hematology analyzer counts individual particles, so clumped platelets are counted as a single event rather than multiple platelets. The result: a falsely low platelet count that looks like severe thrombocytopenia.
The rule: always examine the blood smear before diagnosing thrombocytopenia. If you see platelet clumps at the feathered edge and the rest of the smear looks relatively normal, the analyzer count is unreliable. Recollect if possible. Estimate platelet count from the smear (10 platelets per field at 100x ≈ 100,000 platelets/μL is a useful rough estimate). Do not start expensive diagnostics for thrombocytopenia before ruling out this extremely common artifact.
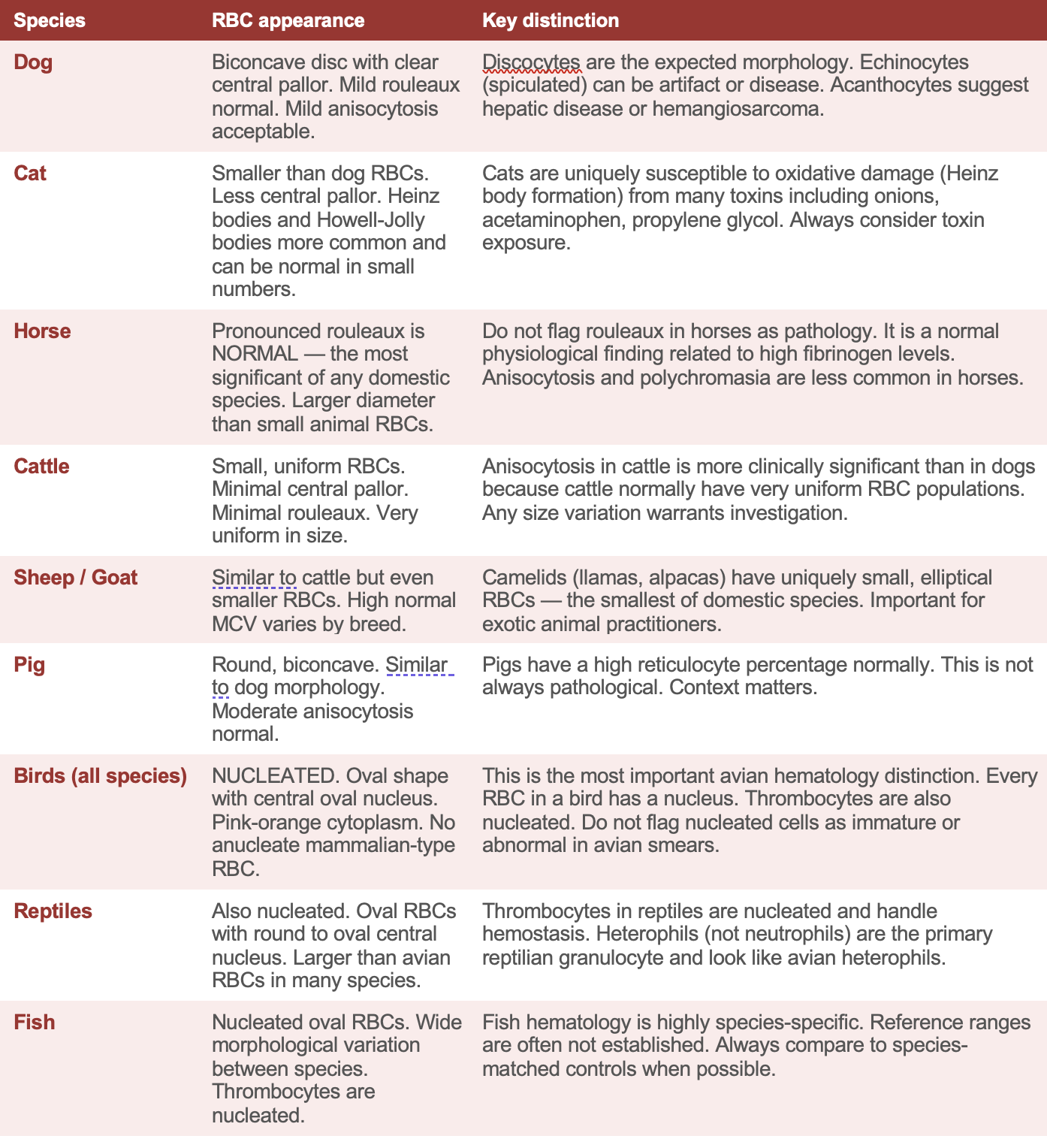
Species-Specific Blood Cell Appearance: The Reference Table
This is the table to have before every blood smear practical. Normal in one species is pathological in another. You need to know the difference before you read a smear, not after.
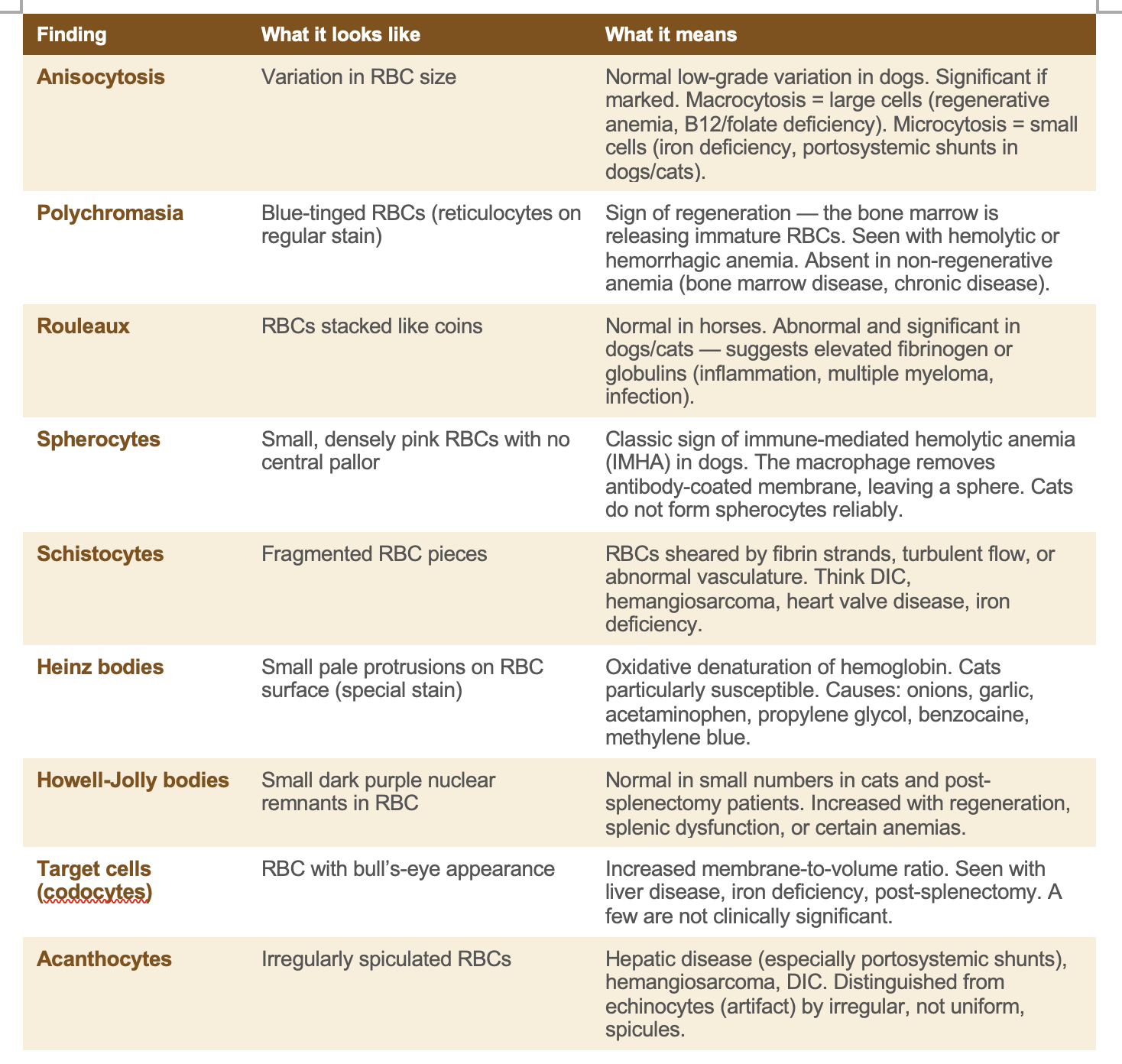
Reading the Smear: RBC Morphological Abnormalities
The following abnormalities will appear repeatedly in your clinical pathology course and in clinical rotations. Each one has a specific appearance and a specific differential diagnosis list. Learn the appearance first, then learn what it means clinically.
Understanding the Complete Blood Count (CBC): What the Numbers Mean
The CBC is the most commonly ordered diagnostic test in veterinary medicine. Understanding what each value represents and how to interpret it in context is a core clinical skill.
CBC PARAMETERS DECODED
PCV / Hematocrit (HCT): The percentage of whole blood that is RBCs. Dog normal ∼ 37–55%. Cat ∼ 25–45%. Low = anemia. High = dehydration (relative) or polycythemia (absolute).
Hemoglobin (Hgb): The oxygen-carrying protein concentration. Roughly 1/3 of the PCV value. More clinically relevant than PCV for assessing oxygen-carrying capacity.
MCV (Mean Corpuscular Volume): Average RBC size. High MCV = macrocytosis (regenerative anemia, B12/folate deficiency, FeLV in cats). Low MCV = microcytosis (iron deficiency, portosystemic shunts).
MCHC (Mean Corpuscular Hemoglobin Concentration): Hemoglobin concentration per RBC. Low MCHC = hypochromia (iron deficiency, regeneration). High MCHC is often an artifact (hemolysis in the sample).
Reticulocyte count: Immature RBCs that still contain residual RNA (appear blue on new methylene blue stain). Elevated reticulocyte count = regenerative response = bone marrow is responding. Important: cats have aggregate and punctate reticulocytes — only aggregate reticulocytes indicate active regeneration.
WBC differential: The percentage of each WBC type. A left shift (bands > mature neutrophils) indicates the marrow is releasing immature cells due to high demand. A regenerative left shift = adequate marrow response. A degenerative left shift (more bands than mature neutrophils with neutropenia) = serious, often grave prognosis.
The Clinical Habit That Separates Good Clinicians
Every experienced clinician in veterinary medicine has a habit that students eventually learn to adopt: look at the blood smear yourself. Do not rely exclusively on the analyzer. Do not accept a platelet count of 15,000 without looking at the smear for clumping. Do not accept a leukocyte differential without checking that the morphology matches the clinical picture.
The analyzer is fast. The smear is true. When they disagree, the smear wins. This is true in a busy emergency practice at 2am and it is true in a specialist referral center with the best equipment available. The smear is the ground truth.
Learn to read smears early. Be slow and systematic at first. Name every cell type you see. Identify the morphological abnormalities. Connect what you see on the slide to what you know about the patient’s history. That connection — between the glass slide and the animal in the cage — is where hematology stops being a lecture topic and starts being a clinical tool.
The analyzer is fast. The smear is true. When they disagree, the smear wins. Look at the smear yourself. Every time. This habit will save patients.
Scrub Squad · Day 5 of 99 · Mind
This article is part of the Scrub Squad 99-day program from Vet Candy. Free for every first-year vet student.