

Sympathetic vs Parasympathetic
The framework that makes the autonomic nervous system actually make sense, plus every drug that touches it
The autonomic nervous system is the part of your nervous system that runs in the background. Heart rate, digestion, pupil size, bladder tone, secretions, blood pressure — none of this requires your conscious attention. It happens because of a finely balanced system of two opposing divisions that spend their entire existence counterbalancing each other.
Most students approach the ANS as a memorization problem. They make two columns, write down a list of effects for each division, and try to hold it all in working memory. This works for about a week and then falls apart under exam pressure, because there is no coherent mental model behind the list.
This article is going to give you the mental model first. Once you have it, the list is not something you memorize. It is something you derive. And derived knowledge survives under pressure in a way that memorized lists do not.
The goal is not to memorize sympathetic and parasympathetic effects. The goal is to understand the logic so clearly that you can derive the effects from first principles. That is the difference between a list that fades and a framework that stays.
The Mental Model: One Scenario, Two States
Imagine an animal being chased by a predator. Every physiological response that helps it survive that moment is sympathetic. Every physiological response that is appropriate for resting, eating, and recovering is parasympathetic.
That single sentence generates almost the entire comparison table. Pupils dilate under sympathetic activation because wide pupils in low light help you detect movement. Heart rate increases because you need blood moving to muscles fast. Digestion slows because blood is redirected away from the gut toward skeletal muscle. Bronchioles dilate because you need maximum oxygen exchange. The bladder relaxes because this is not the moment.
Parasympathetic is the opposite state. Pupils constrict because the threat has passed and you are focusing on your plate. Heart rate decreases because you are resting. Digestion increases because now is the time to process food. Bronchioles constrict to normal diameter. The bladder is allowed to void. Salivary glands produce copious watery secretion to begin chemical digestion.
Once you internalize fight-or-flight versus rest-and-digest as two coherent physiological states, every individual effect becomes a logical consequence of one of those states rather than an isolated fact to memorize.
Pupils dilating under sympathetic activation is not an arbitrary fact. Wide pupils in low light help you detect a predator. Every sympathetic effect makes sense if you ask: does this help an animal survive a threat?
The Anatomy: Where Each Division Comes From
Sympathetic: Thoracolumbar
Sympathetic preganglionic neurons originate in the lateral horn of the spinal cord from approximately T1 to L2 or L3, depending on the species. This is called the thoracolumbar outflow. Preganglionic fibers exit the spinal cord with the ventral roots and travel to one of two types of ganglia: the paravertebral sympathetic chain ganglia (which run alongside the vertebral column like a string of beads) or the prevertebral ganglia (celiac, cranial mesenteric, caudal mesenteric), which lie in the abdomen near the major vessels.
A critical anatomical feature of the sympathetic division is that its ganglia are far from the target organs. This means preganglionic fibers are short and postganglionic fibers are long. The postganglionic neurons release norepinephrine at the target organ, which binds to adrenergic receptors (alpha and beta subtypes). The one major exception is sweat glands, which have sympathetic innervation but use acetylcholine rather than norepinephrine at the effector — this is a classic exam trap.
The adrenal medulla is a modified sympathetic ganglion. Preganglionic sympathetic fibers bypass the paravertebral ganglia and synapse directly on chromaffin cells in the adrenal medulla, which then release epinephrine (80%) and norepinephrine (20%) directly into the bloodstream. This is why a major sympathetic activation — such as the stress response — produces a systemic hormonal effect, not just a localized neural one.
Parasympathetic: Craniosacral
Parasympathetic preganglionic neurons originate in two locations: the brainstem (cranial division, via CN III, VII, IX, and X) and the sacral spinal cord (S2-S4). This is called the craniosacral outflow. The vagus nerve (CN X) is by far the most significant contributor — it provides parasympathetic innervation to the heart, lungs, esophagus, stomach, small intestine, and most of the large intestine as far as the splenic flexure.
The defining anatomical feature of the parasympathetic division is that its ganglia are near or within the target organs. This means preganglionic fibers are long and postganglionic fibers are short. Postganglionic neurons release acetylcholine at the effector, which binds to muscarinic receptors. Muscarinic receptors are the ones blocked by atropine — which is why atropine increases heart rate, dilates pupils, and reduces secretions.
The four cranial nerve contributions and their targets: CN III (oculomotor) → pupillary constriction and lens accommodation via ciliary ganglion. CN VII (facial) → lacrimal, submandibular, and sublingual glands. CN IX (glossopharyngeal) → parotid gland via otic ganglion. CN X (vagus) → thoracic and abdominal viscera.
The Neurotransmitters: Two Synapses, Two Options
Both divisions use acetylcholine at the ganglion (at nicotinic receptors, which is why nicotine produces both sympathetic and parasympathetic effects simultaneously and why you get a complex mix of cardiovascular effects from nicotine exposure).
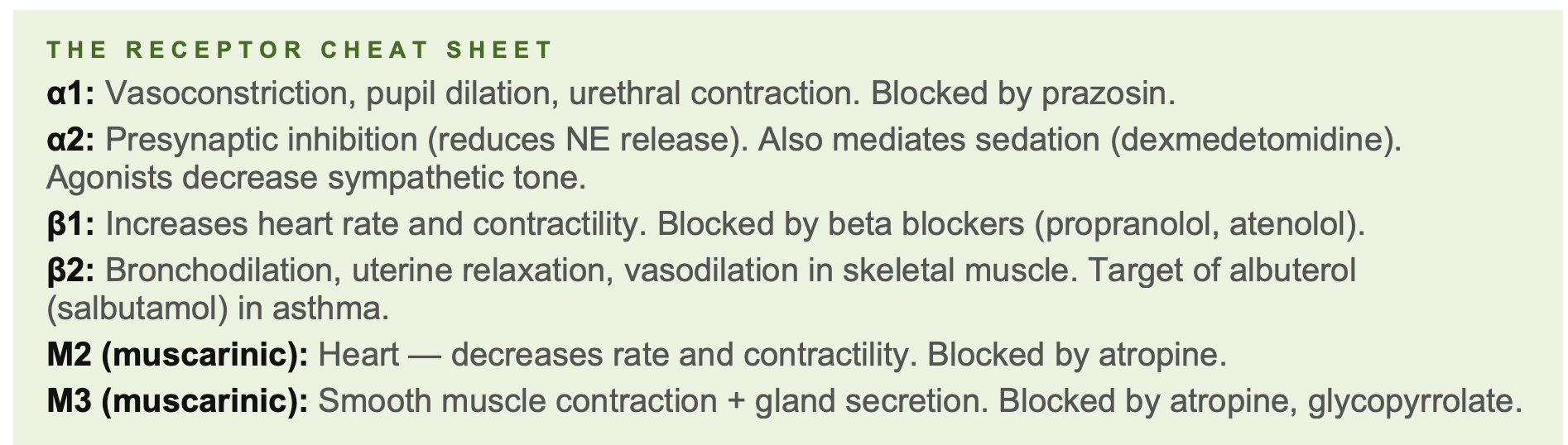
At the target organ, the divisions diverge. Sympathetic postganglionic neurons release norepinephrine, which binds to adrenergic receptors. Alpha-1 receptors mediate vasoconstriction and pupil dilation. Alpha-2 receptors are presynaptic inhibitory receptors. Beta-1 receptors increase heart rate and contractility. Beta-2 receptors dilate bronchioles and relax uterine muscle. Beta-3 receptors mediate lipolysis in fat tissue.
Parasympathetic postganglionic neurons release acetylcholine at muscarinic receptors. There are five muscarinic subtypes (M1–M5), but for first year the key ones are M2 (heart — decreases rate and contractility) and M3 (smooth muscle and glands — contracts visceral smooth muscle, increases secretions).
THE RECEPTOR CHEAT SHEET
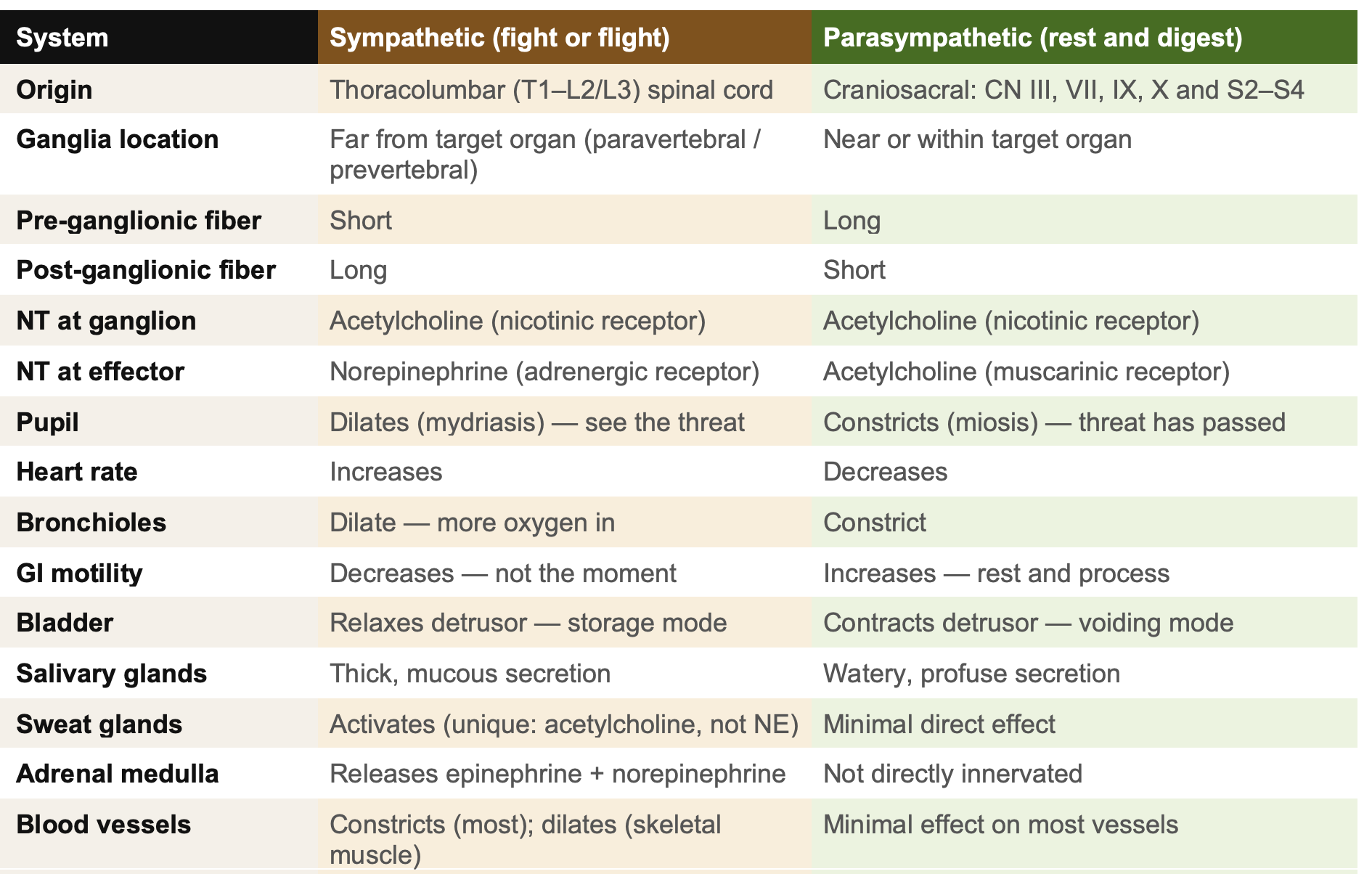
The Full Comparison Table
Amber = sympathetic. Green = parasympathetic. The color coding maps to the fight-or-flight (warm, urgent) versus rest-and-digest (cool, calm) framework.
Clinical Applications: What This Looks Like in a Patient
Horner’s Syndrome
Horner’s syndrome results from disruption of the sympathetic innervation to the eye and face on one side. Because the sympathetic pathway to the eye is a three-neuron pathway, the location of the lesion can be localized by pharmacological testing.
The classic signs are: miosis (small pupil — parasympathetic is unopposed and constricts it), ptosis (drooping upper eyelid — the superior tarsal muscle is sympathetically innervated), enophthalmos (eyeball appears sunken — the retractor bulbi and orbital smooth muscle lose tone), and in some species protrusion of the third eyelid. Anhydrosis (lack of sweating on the ipsilateral side of the face) occurs in animals that sweat facially.
In dogs, Horner’s syndrome is commonly caused by: otitis media/interna (affecting the middle ear, where the postganglionic sympathetic fiber travels close to the tympanic bulla), brachial plexus injury, cranial mediastinal masses, or spinal cord lesions between T1 and T3.
Pharmacological localization: applying 10% phenylephrine to the affected eye and timing how long it takes to dilate the pupil can help localize the lesion. Postganglionic lesions dilate fastest (within 20 minutes) because of denervation supersensitivity. Preganglionic lesions take longer (45–60 minutes). Central lesions show minimal or no response. Pilocarpine 1% (parasympathomimetic) is used as an alternative localization test.
Vagal Tone and Cardiovascular Effects
The vagus nerve is the primary determinant of resting heart rate in most mammals. Athletes and very fit animals have higher vagal tone and therefore lower resting heart rates. This is a normal physiological finding, not pathology.
Vasovagal syncope occurs when an exaggerated vagal response causes sudden bradycardia and hypotension, leading to transient loss of consciousness. In veterinary medicine, this can be triggered by respiratory distress, pain, excitement, or tracheal compression. Carotid sinus massage (gently compressing the carotid body, which is rich in baroreceptors that trigger vagal activation) can be used diagnostically and therapeutically in some tachyarrhythmias.
Atropine is the antidote for excessive vagal tone or parasympathetic poisoning because it blocks muscarinic receptors, preventing acetylcholine from slowing the heart. The atropine response test in dogs (0.04 mg/kg IV) is used to differentiate vagal-mediated bradycardia (responds with tachycardia) from intrinsic cardiac disease (no response or inadequate response).
Organophosphate and Carbamate Toxicity
Organophosphate and carbamate compounds inhibit acetylcholinesterase, the enzyme that breaks down acetylcholine. With AChE inhibited, acetylcholine accumulates at all cholinergic synapses simultaneously — which means massive stimulation of both muscarinic and nicotinic receptors throughout the body.
The clinical syndrome is remembered by two mnemonics. DUMBELS covers the muscarinic effects: Defecation, Urination, Miosis, Bradycardia, Emesis, Lacrimation, Salivation. SLUDE is another: Salivation, Lacrimation, Urination, Defecation, Emesis. Nicotinic effects (at the neuromuscular junction and sympathetic ganglia) produce muscle fasciculations, weakness, and eventually paralysis.
Treatment has two components: atropine (blocks the muscarinic effects only — give to effect, targeting dry secretions and normal heart rate, not pupil dilation) plus pralidoxime (2-PAM) for organophosphates specifically, which can reactivate AChE if given before aging occurs. Carbamates do not benefit from pralidoxime. Supportive care and seizure management are critical
Atropine in OP toxicity controls the DUMBELS syndrome but does not reverse muscle paralysis (nicotinic effect). Pralidoxime treats the cause. If you mix them up on an exam or a rotation, the patient pays for it. Know the distinction.
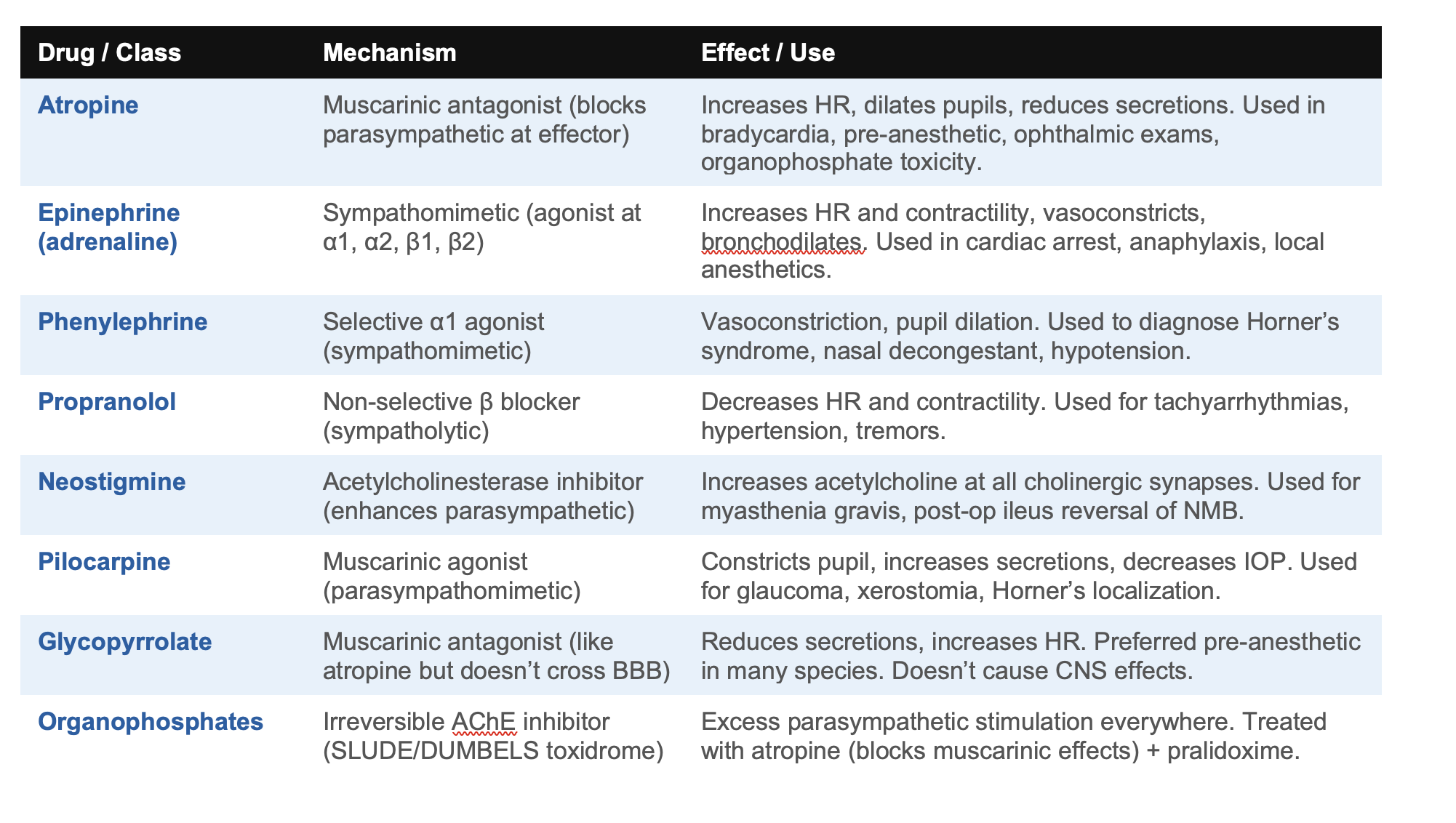
The Drug Table: Everything That Touches the ANS
Every drug in this table will appear in your pharmacology course. Most will appear in your clinical rotations. Understanding why each one works — not just what it does — is the difference between a student who looks up doses and a clinician who understands mechanisms.
The Mnemonics Worth Keeping
MEMORIZE THESE. THEY ACTUALLY WORK.
Fight or flight vs Rest and digest: The master mnemonic. Every effect follows from one of these two states.
DUMBELS (parasympathetic overstimulation): Defecation, Urination, Miosis, Bradycardia, Emesis, Lacrimation, Salivation. Think: a very wet, very unhappy patient.
SLUD (parasympathetic signs): Salivation, Lacrimation, Urination, Defecation. Shorter version of the same mnemonic.
Sympathetic speeds, Parasympathetic pumps the brakes: HR, GI motility, bronchiole diameter — all faster/bigger under sympathetic, all slower/smaller under parasympathetic.
Atropine = anti-SLUD: Atropine blocks muscarinic receptors = blocks all parasympathetic effects at effector organs. Dry, fast, big pupils.
Sweat glands are the exception: Sympathetically innervated but use ACh (muscarinic) not NE. Atropine therefore reduces sweating even though sweating is a sympathetic response.
Ganglionic NT is always ACh (nicotinic): Both divisions. Nicotine stimulates both. This is why nicotine produces mixed cardiovascular effects.
Why Dr. Tracy Is Right: Localization Over Memorization
Dr. Gaemia Tracy’s advice applies directly here. You do not need to memorize a list of sympathetic and parasympathetic effects. You need to understand the two states so well that every specific effect is derivable from the logic.
When you see a patient with miosis, ptosis, and enophthalmos on one side, you do not flip through a mental database of clinical signs. You ask: which division is overriding the other? The answer is parasympathetic. Which structure was damaged to allow that? The sympathetic pathway to the eye. Where along the three-neuron pathway is the lesion? That depends on the history and the pharmacological localization test.
That is the localization approach in practice. The ANS framework is not a memorization task. It is the scaffolding on which every cardiology, neurology, toxicology, and pharmacology case you will encounter for the next four years will hang. Build it properly now. You will use it every day.
You are going to encounter the autonomic nervous system in every pharmacology lecture, every cardiovascular case, every toxicology consult, and every neurological exam for the rest of your career. The time you invest in understanding it now is one of the highest-return investments you will make in year one.
Scrub Squad · Day 4 of 99 · Mind
This article is part of the Scrub Squad 99-day program from Vet Candy. Free for every first-year vet student.